00016126302019FYfalse--12-310.0010.00150,00050,000————0.0010.00120,000,00020,000,00013,898,69413,757,20013,882,93213,742,53015,76214,670P3YP3Y111113,344,25835551.892.612.532.9P5Y00016126302019-01-012019-12-31iso4217:USD00016126302019-06-28xbrli:shares00016126302020-03-0300016126302019-12-3100016126302018-12-31iso4217:USDxbrli:shares0001612630jynt:RevenuesAndManagementFeesFromCompanyClinicsMember2019-01-012019-12-310001612630jynt:RevenuesAndManagementFeesFromCompanyClinicsMember2018-01-012018-12-310001612630us-gaap:RoyaltyMember2019-01-012019-12-310001612630us-gaap:RoyaltyMember2018-01-012018-12-310001612630us-gaap:FranchiseMember2019-01-012019-12-310001612630us-gaap:FranchiseMember2018-01-012018-12-310001612630us-gaap:AdvertisingMember2019-01-012019-12-310001612630us-gaap:AdvertisingMember2018-01-012018-12-310001612630us-gaap:TechnologyServiceMember2019-01-012019-12-310001612630us-gaap:TechnologyServiceMember2018-01-012018-12-310001612630jynt:RegionalDeveloperFeesMember2019-01-012019-12-310001612630jynt:RegionalDeveloperFeesMember2018-01-012018-12-310001612630us-gaap:ProductAndServiceOtherMember2019-01-012019-12-310001612630us-gaap:ProductAndServiceOtherMember2018-01-012018-12-3100016126302018-01-012018-12-310001612630us-gaap:CommonStockMember2017-12-310001612630us-gaap:AdditionalPaidInCapitalMember2017-12-310001612630us-gaap:TreasuryStockMember2017-12-310001612630us-gaap:RetainedEarningsMember2017-12-310001612630us-gaap:ParentMember2017-12-310001612630us-gaap:NoncontrollingInterestMember2017-12-3100016126302017-12-310001612630us-gaap:AdditionalPaidInCapitalMember2018-01-012018-12-310001612630us-gaap:ParentMember2018-01-012018-12-310001612630us-gaap:CommonStockMember2018-01-012018-12-310001612630us-gaap:TreasuryStockMember2018-01-012018-12-310001612630us-gaap:RetainedEarningsMember2018-01-012018-12-310001612630us-gaap:CommonStockMember2018-12-310001612630us-gaap:AdditionalPaidInCapitalMember2018-12-310001612630us-gaap:TreasuryStockMember2018-12-310001612630us-gaap:RetainedEarningsMember2018-12-310001612630us-gaap:ParentMember2018-12-310001612630us-gaap:NoncontrollingInterestMember2018-12-310001612630us-gaap:RetainedEarningsMember2019-01-012019-12-310001612630us-gaap:ParentMember2019-01-012019-12-310001612630us-gaap:AdditionalPaidInCapitalMember2019-01-012019-12-310001612630us-gaap:CommonStockMember2019-01-012019-12-310001612630us-gaap:TreasuryStockMember2019-01-012019-12-310001612630us-gaap:CommonStockMember2019-12-310001612630us-gaap:AdditionalPaidInCapitalMember2019-12-310001612630us-gaap:TreasuryStockMember2019-12-310001612630us-gaap:RetainedEarningsMember2019-12-310001612630us-gaap:ParentMember2019-12-310001612630us-gaap:NoncontrollingInterestMember2019-12-310001612630jynt:PurchaseOfPropertyPlantAndEquipmentIncludedInAccountsPayableMember2019-01-012019-12-310001612630jynt:PurchaseOfPropertyPlantAndEquipmentIncludedInAccruedExpensesMember2019-01-012019-12-310001612630jynt:PurchaseOfPropertyPlantAndEquipmentIncludedInAccountsPayableMember2018-01-012018-12-310001612630jynt:PurchaseOfPropertyPlantAndEquipmentIncludedInAccruedExpensesMember2018-01-012018-12-310001612630jynt:AssetsAndFranchiseAgreementMember2019-12-310001612630jynt:LicenseFeeCollectionUponRegionalDeveloperAgreementMember2019-12-310001612630srt:ScenarioPreviouslyReportedMemberjynt:RevenuesAndManagementFeesFromCompanyClinicsMember2018-01-012018-12-310001612630jynt:RevenuesAndManagementFeesFromCompanyClinicsMembersrt:RestatementAdjustmentMember2018-01-012018-12-310001612630srt:ScenarioPreviouslyReportedMember2018-01-012018-12-310001612630srt:RestatementAdjustmentMember2018-01-012018-12-310001612630srt:ScenarioPreviouslyReportedMember2018-12-310001612630srt:RestatementAdjustmentMember2018-12-310001612630us-gaap:FranchiseMembersrt:RestatementAdjustmentMember2019-10-012019-12-31jynt:clinic0001612630us-gaap:FranchisedUnitsMember2018-12-310001612630us-gaap:FranchisedUnitsMember2017-12-310001612630us-gaap:FranchisedUnitsMember2019-01-012019-12-310001612630us-gaap:FranchisedUnitsMember2018-01-012018-12-310001612630us-gaap:FranchisedUnitsMember2019-12-310001612630us-gaap:EntityOperatedUnitsMember2018-12-310001612630us-gaap:EntityOperatedUnitsMember2017-12-310001612630us-gaap:EntityOperatedUnitsMember2019-01-012019-12-310001612630us-gaap:EntityOperatedUnitsMember2018-01-012018-12-310001612630us-gaap:EntityOperatedUnitsMember2019-12-310001612630srt:MinimumMember2019-01-012019-12-310001612630srt:MaximumMember2019-01-012019-12-310001612630us-gaap:ComputerSoftwareIntangibleAssetMember2019-01-012019-12-310001612630us-gaap:FranchiseRightsMembersrt:MinimumMember2019-01-012019-12-310001612630us-gaap:FranchiseRightsMembersrt:MaximumMember2019-01-012019-12-310001612630jynt:DevelopmentRightsMember2019-01-012019-12-310001612630us-gaap:CustomerRelationshipsMember2019-01-012019-12-31xbrli:purejynt:agreement0001612630jynt:RegionalDevelopmentAgreementMember2019-12-310001612630jynt:RegionalDevelopmentAgreementMember2018-12-310001612630us-gaap:RestrictedStockMember2019-01-012019-12-310001612630us-gaap:RestrictedStockMember2018-01-012018-12-310001612630us-gaap:EmployeeStockOptionMember2019-01-012019-12-310001612630us-gaap:EmployeeStockOptionMember2018-01-012018-12-31jynt:franchise0001612630jynt:AssetsAndFranchiseAgreementMember2019-03-180001612630jynt:AssetsAndFranchiseAgreementMember2019-03-182019-03-180001612630jynt:AssetsAndFranchiseAgreementMember2019-07-090001612630jynt:AssetsAndFranchiseAgreementMember2019-07-092019-07-090001612630jynt:AssetsAndFranchiseAgreementMember2019-07-170001612630jynt:AssetsAndFranchiseAgreementMember2019-07-172019-07-170001612630jynt:AssetsAndFranchiseAgreementMember2019-08-010001612630jynt:AssetsAndFranchiseAgreementMember2019-08-012019-08-010001612630jynt:AssetsAndFranchiseAgreementMember2019-08-150001612630jynt:AssetsAndFranchiseAgreementMember2019-08-152019-08-150001612630jynt:AssetsAndFranchiseAgreementMember2019-10-280001612630jynt:AssetsAndFranchiseAgreementMember2019-10-282019-10-280001612630jynt:AssetsAndFranchiseAgreementMember2019-01-012019-12-310001612630jynt:AssetsAndFranchiseAgreementMemberus-gaap:FranchiseRightsMember2019-12-310001612630jynt:AssetsAndFranchiseAgreementMemberus-gaap:FranchiseRightsMember2019-01-012019-12-310001612630jynt:AssetsAndFranchiseAgreementMemberus-gaap:CustomerRelationshipsMember2019-12-310001612630jynt:AssetsAndFranchiseAgreementMemberus-gaap:CustomerRelationshipsMember2019-01-012019-12-310001612630jynt:AssetsAndFranchiseAgreementMember2018-01-012018-12-31jynt:state00016126302020-01-012019-12-3100016126302021-01-012019-12-3100016126302022-01-012019-12-3100016126302023-01-012019-12-3100016126302024-01-012019-12-3100016126302025-01-012019-12-310001612630jynt:RegionalDeveloperTerritoryInCentralFloridaMember2017-04-290001612630jynt:RegionalDeveloperTerritoryInCentralFloridaMemberjynt:The10PercentInterestBearingPromissoryNoteMaturingOctober12020Member2017-04-290001612630jynt:RegionalDeveloperTerritoryInCentralFloridaMemberjynt:The10PercentInterestBearingPromissoryNoteMaturingOctober12020Member2017-04-292017-04-290001612630jynt:RegionalDeveloperTerritoryInMarylandwashingtonDCMember2017-08-310001612630jynt:The10PercentInterestBearingPromissoryNoteMaturingAugust12020Memberjynt:RegionalDeveloperTerritoryInMarylandwashingtonDCMember2017-08-310001612630jynt:The10PercentInterestBearingPromissoryNoteMaturingAugust12020Memberjynt:RegionalDeveloperTerritoryInMarylandwashingtonDCMember2017-08-312017-08-310001612630jynt:RegionalDeveloperTerritoryInMinnesotaMember2017-09-220001612630jynt:The10PercentInterestBearingPromissoryNoteMaturingSeptember12020Memberjynt:RegionalDeveloperTerritoryInMinnesotaMember2017-09-220001612630jynt:The10PercentInterestBearingPromissoryNoteMaturingSeptember12020Memberjynt:RegionalDeveloperTerritoryInMinnesotaMember2017-09-012017-09-220001612630jynt:RegionalDeveloperTerritoriesWithTexasArkansasAndOklahomaMember2017-10-100001612630jynt:InterestBearingPromissoryNoteMaturingOctober242020Memberjynt:RegionalDeveloperTerritoriesWithTexasArkansasAndOklahomaMember2017-10-100001612630jynt:InterestBearingPromissoryNoteMaturingOctober242020Memberjynt:RegionalDeveloperTerritoriesWithTexasArkansasAndOklahomaMember2017-10-102017-10-1000016126302019-04-2600016126302019-04-262019-04-260001612630jynt:CompanyOwnedClinicMember2019-12-310001612630jynt:CompanyOwnedClinicMember2018-12-310001612630us-gaap:OfficeEquipmentMember2019-12-310001612630us-gaap:OfficeEquipmentMember2018-12-310001612630us-gaap:LeaseholdImprovementsMember2019-12-310001612630us-gaap:LeaseholdImprovementsMember2018-12-310001612630us-gaap:SoftwareDevelopmentMember2019-12-310001612630us-gaap:SoftwareDevelopmentMember2018-12-310001612630jynt:LeasedAssetsMember2019-12-310001612630jynt:PropertyPlantAndEquipmentExcludingConstructionInProgressMember2019-12-310001612630jynt:PropertyPlantAndEquipmentExcludingConstructionInProgressMember2018-12-310001612630jynt:RegionalDeveloperRightsInSouthCarolinaAndGeorgiaMember2019-02-040001612630jynt:RegionalDeveloperRightsInSouthCarolinaAndGeorgiaMember2019-02-042019-02-040001612630us-gaap:FranchiseRightsMember2019-12-310001612630us-gaap:CustomerRelationshipsMember2019-12-310001612630jynt:DevelopmentRightsMember2019-12-310001612630us-gaap:FranchiseRightsMember2018-12-310001612630us-gaap:CustomerRelationshipsMember2018-12-310001612630jynt:DevelopmentRightsMember2018-12-31jynt:note00016126302016-01-012016-12-310001612630jynt:NotesPayableDeliveredAsAPortionOfTheConsiderationPaidInConnectionWithAcquisitionsMember2016-12-310001612630us-gaap:RevolvingCreditFacilityMember2017-01-030001612630us-gaap:RevolvingCreditFacilityMember2017-01-032017-01-030001612630us-gaap:RevolvingCreditFacilityMember2019-12-310001612630us-gaap:LineOfCreditMemberus-gaap:SecuredDebtMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-290001612630us-gaap:RevolvingCreditFacilityMemberus-gaap:LineOfCreditMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-290001612630jynt:DevelopmentLineOfCreditMemberus-gaap:LineOfCreditMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-290001612630us-gaap:EmployeeStockOptionMember2019-01-012019-12-310001612630us-gaap:EmployeeStockOptionMember2018-01-012018-12-310001612630us-gaap:EmployeeStockOptionMember2017-12-310001612630us-gaap:EmployeeStockOptionMember2017-01-012017-12-310001612630us-gaap:EmployeeStockOptionMember2018-12-310001612630us-gaap:EmployeeStockOptionMember2019-12-31jynt:installment0001612630us-gaap:RestrictedStockMember2019-12-310001612630us-gaap:RestrictedStockMember2018-12-310001612630us-gaap:RestrictedStockMember2019-01-012019-12-310001612630us-gaap:RestrictedStockMember2018-01-012018-12-310001612630us-gaap:IPOMember2015-11-102018-11-100001612630us-gaap:IPOMember2018-11-100001612630srt:MinimumMemberus-gaap:EmployeeStockOptionMember2019-01-012019-12-310001612630srt:MaximumMemberus-gaap:EmployeeStockOptionMember2019-01-012019-12-310001612630srt:MinimumMemberus-gaap:EmployeeStockOptionMember2018-01-012018-12-310001612630srt:MaximumMemberus-gaap:EmployeeStockOptionMember2018-01-012018-12-310001612630us-gaap:DomesticCountryMember2019-12-310001612630us-gaap:StateAndLocalJurisdictionMember2019-12-310001612630us-gaap:ResearchMember2019-12-310001612630jynt:CaliforniaAlternativeMinimumTaxCreditMember2019-12-310001612630srt:MinimumMember2019-12-310001612630srt:MaximumMember2019-12-31jynt:segment0001612630jynt:CorporateClinicsMember2019-01-012019-12-310001612630jynt:CorporateClinicsMember2018-01-012018-12-310001612630jynt:FranchiseOperationsMember2019-01-012019-12-310001612630jynt:FranchiseOperationsMember2018-01-012018-12-310001612630jynt:CorporateClinicsMemberus-gaap:OperatingSegmentsMember2019-01-012019-12-310001612630jynt:CorporateClinicsMemberus-gaap:OperatingSegmentsMember2018-01-012018-12-310001612630jynt:FranchiseOperationsMemberus-gaap:OperatingSegmentsMember2019-01-012019-12-310001612630jynt:FranchiseOperationsMemberus-gaap:OperatingSegmentsMember2018-01-012018-12-310001612630us-gaap:OperatingSegmentsMember2019-01-012019-12-310001612630us-gaap:OperatingSegmentsMember2018-01-012018-12-310001612630us-gaap:CorporateMember2019-01-012019-12-310001612630us-gaap:CorporateMember2018-01-012018-12-310001612630us-gaap:CorporateNonSegmentMember2019-01-012019-12-310001612630us-gaap:CorporateNonSegmentMember2018-01-012018-12-310001612630jynt:CorporateClinicsMemberus-gaap:OperatingSegmentsMember2019-12-310001612630jynt:CorporateClinicsMemberus-gaap:OperatingSegmentsMember2018-12-310001612630jynt:FranchiseOperationsMemberus-gaap:OperatingSegmentsMember2019-12-310001612630jynt:FranchiseOperationsMemberus-gaap:OperatingSegmentsMember2018-12-310001612630us-gaap:OperatingSegmentsMember2019-12-310001612630us-gaap:OperatingSegmentsMember2018-12-310001612630us-gaap:LineOfCreditMemberus-gaap:SecuredDebtMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-280001612630us-gaap:RevolvingCreditFacilityMemberus-gaap:LineOfCreditMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-280001612630jynt:DevelopmentLineOfCreditMemberus-gaap:LineOfCreditMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-280001612630us-gaap:LineOfCreditMemberus-gaap:LetterOfCreditMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-28jynt:payment0001612630us-gaap:EurodollarMemberus-gaap:LineOfCreditMemberus-gaap:SecuredDebtMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-282020-02-280001612630us-gaap:LineOfCreditMemberus-gaap:SecuredDebtMemberjynt:AlternativeBaseRateMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-282020-02-280001612630us-gaap:LineOfCreditMemberus-gaap:SecuredDebtMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:PrimeRateMemberus-gaap:SubsequentEventMember2020-02-282020-02-280001612630us-gaap:LineOfCreditMemberjynt:AlternativeEurocurrencyBaseRateMemberjynt:SeniorSecuredCreditFacilitiesMemberus-gaap:SubsequentEventMember2020-02-282020-02-28
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| | | | | |
| ☒ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2019
OR
| | | | | |
| ☐ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from _______ to ________
Commission File Number: 001-36724
The Joint Corp.
(Exact name of registrant as specified in its charter)
| | | | | |
| Delaware | 90-0544160 |
(State or Other Jurisdiction of Incorporation) | (I.R.S. Employer Identification No.) |
| | | | | |
16767 North Perimeter Drive, Suite 110, Scottsdale, Arizona | 85260 |
| (Address of Principal Executive Offices) | (Zip Code) |
(480) 245-5960
(Registrant’s Telephone Number, Including Area Code)
Securities registered pursuant to Section 12(b) of the Act:
| | | | | | | | |
| Trading | |
| Title Of Each Class | Symbol(s) | Name Of Each Exchange On Which Registered |
| Common Stock, $0.001 Par Value Per Share | JYNT | The NASDAQ Capital Market LLC |
Securities Registered Pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☑
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☑
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☑ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☑ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| | | | | |
Large accelerated filer ☐ | Accelerated filer ☑ |
Non-accelerated filer ☐ | Smaller reporting company ☑ |
| Emerging growth company ☐ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐ No ☑
The aggregate market value of the voting and non-voting common equity held by non-affiliates of the registrant was approximately $236.4 million as of June 28, 2019 based on the closing sales price of the common stock on the NASDAQ Capital Market.
There were 13,882,932 shares of the registrant’s common stock outstanding as of March 3, 2020.
Documents Incorporated by Reference
Portions of the registrant's Proxy Statement relating to its 2020 Annual Meeting of Stockholders, to be filed with the Securities and Exchange Commission (“SEC”) pursuant to Regulation 14A within 120 days after the registrant’s fiscal year ended December 31, 2019, are incorporated by reference in Part III of this Form 10-K.
TABLE OF CONTENTS
Forward-Looking Statements and Terminology
The information in this Annual Report on Form 10-K, or this Form 10-K, including this discussion under the headings “Business” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” contains forward-looking statements and information within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended, or the Exchange Act, which are subject to the “safe harbor” created by those sections. All statements, other than statements of historical facts, included or incorporated in this Form 10-K could be deemed forward-looking statements, particularly statements about our plans, strategies and prospects under the headings “Business” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” In some cases, you can identify forward-looking statements by terminology such as “may,” “will,” “should,” “could,” “expects,” “plans,” “anticipates,” “believes,” “estimates,” “predicts,” “potential,” “continue,” “intend” or the negative of these terms or other comparable terminology. All forward-looking statements in this Form 10-K are made based on our current expectations, forecasts, estimates and assumptions, and involve risks, uncertainties and other factors that could cause results or events to differ materially from those expressed in the forward-looking statements. In evaluating these statements, you should specifically consider various factors, uncertainties and risks that could affect our future results or operations as described from time to time in our SEC reports, including those risks outlined under “Risk Factors” in Item 1A of this Form 10-K. These factors, uncertainties and risks may cause our actual results to differ materially from any forward-looking statement set forth in this Form 10-K. You should carefully consider the trends, risks and uncertainties described below and other information in this Form 10-K and subsequent reports filed with or furnished to the SEC before making any investment decision with respect to our securities. All forward-looking statements attributable to us or persons acting on our behalf are expressly qualified in their entirety by this cautionary statement. Some of the important factors that could cause our actual results to differ materially from those projected in any forward-looking statements include, but are not limited to, the following:
•we may not be able to successfully implement our growth strategy if we or our franchisees are unable to locate and secure appropriate sites for clinic locations, obtain favorable lease terms, and attract patients to our clinics;
•we have limited experience operating company-owned or managed clinics, and we may not be able to duplicate the success of some of our franchisees;
•we may not be able to acquire operating clinics from existing franchisees or develop company-owned or managed clinics on attractive terms;
•we may fail to successfully design and maintain our proprietary and third-party management information systems or implement new systems;
•we may fail to properly maintain the integrity of our data or to strategically implement, upgrade or consolidate existing information systems;
•As we increase the number of franchisee acquisitions that we make, it could disrupt our business and harm our financial condition;
•we may not be able to continue to sell regional developer licenses to qualified regional developers or sell franchises to qualified franchisees, and our regional developers and franchisees may not succeed in developing profitable territories and clinics;
•we may not be able to identify, recruit and train enough qualified chiropractors to staff our clinics;
•new clinics may not reach the point of profitability, and we may not be able to maintain or improve revenues and franchise fees from existing franchised clinics;
•the chiropractic industry is highly competitive, with many well-established independent competitors, which could prevent us from increasing our market share or result in reduction in our market share;
•major public health concerns, including the outbreak of the coronavirus, may adversely affect revenue at our clinics and disrupt financial markets, adversely affecting our stock price;
•administrative actions and rulings regarding the corporate practice of medicine and joint employer responsibility may jeopardize our business model;
•we may face negative publicity or damage to our reputation, which could arise from concerns expressed by opponents of chiropractic and by chiropractors operating under traditional service models;
•our security systems may be breached, and we may face civil liability and public perception of our security measures could be diminished, either of which would negatively affect our ability to attract and retain patients;
•legislation, regulations, as well as new medical procedures and techniques could reduce or eliminate our competitive advantages; and
•we face increased costs as a result of being a public company.
Additionally, there may be other risks that are otherwise described from time to time in the reports that we file with the Securities and Exchange Commission. Any forward-looking statements in this report should be considered in light of various important factors, including the risks and uncertainties listed above, as well as others.
As used in this Form 10-K:
•“we,” “us,” and “our” refer to The Joint Corp., its variable interest entities (“VIEs”), and, its wholly owned subsidiary, The Joint Corporate Unit No. 1, LLC, collectively.
•a “clinic” refers to a chiropractic clinic operating under our “Joint” brand, which may be (i) owned by a franchisee, (ii) owned by a professional corporation or limited liability company and managed by a franchisee; (iii) owned directly by us; or (iv) owned by a professional corporation or limited liability company and managed by us.
•when we identify an “operator” of a clinic, a party that is “operating” a clinic, or a party by whom a clinic is “operated,” we are referring to the party that operates all aspects of the clinic in certain jurisdictions, and to the party that manages all aspects of the clinic other than the practice of chiropractic in certain other jurisdictions.
•when we describe our acquisition or our opening of a clinic, we are referring to our acquisition or opening of the entity that operates all aspects of the clinic in certain jurisdictions, and to our acquisition or opening of the entity that manages aspects of the clinic other than the practice of chiropractic in certain other jurisdictions.
PART I
ITEM 1. BUSINESS
| | |
"Our mission is to improve quality of life through routine and affordable chiropractic care." |
Overview
Our principal business is to develop, own, operate, support and manage chiropractic clinics through direct ownership, management arrangements, franchising and the sale of regional developer rights throughout the United States.
We are a rapidly growing franchisor and operator of chiropractic clinics that uses a private pay, non-insurance, cash-based model. We seek to be the leading provider of chiropractic care in the markets we serve and to become the most recognized brand in our industry through the rapid and focused expansion of chiropractic clinics in key markets throughout North America and potentially abroad. We strive to accomplish our mission by making quality care readily available and affordable in a retail setting. We have created a growing network of modern, consumer-friendly chiropractic clinics operated or managed by franchisees and by us that employ licensed chiropractors. Our model enables us to price our services below most competitors’ pricing for similar services and below most insurance co-payment levels (i.e., below the patient co-payment required for an insurance-covered service).
Since acquiring the predecessor to our company in March 2010, we have grown our enterprise from eight to 513 clinics in operation as of December 31, 2019, with an additional 170 franchise licenses sold but not yet developed across our network, and 34 letters-of-intent for future clinic licenses. As of December 31, 2019, 453 of our clinics were operated or managed by franchisees and 60 clinics were operated as company-owned or managed clinics. In the year ended December 31, 2019, our system registered approximately 7.7 million patient visits and generated system-wide sales of $220.3 million. Our future growth strategy remains focused on accelerating the development of our franchise base through the sale of additional franchises and through a robust regional developer network. In 2020, we plan to continue our acceleration of the expansion of our company-owned or managed portfolio through the opportunistic acquisition of select operating clinics or the development of new clinics in areas in which we already support company-owned or managed clinics. We collect a royalty of 7.0% of revenues from franchised clinics. We remit a 3.0% royalty to our regional developers on the gross sales of franchises opened within certain regional developer protected territories. We also collect a national marketing fee of 2.0% of gross sales of all franchised clinics. We receive a franchise sales fee of $39,900 for each franchise we sell directly. For each franchise sold through our network of regional developers, the regional developer typically receives up to 50% of the respective franchise fee. If a franchisee purchases additional franchise licenses, the initial franchise fee is reduced by $10,000 per additional license.
On November 14, 2014, we completed our initial public offering, or the IPO, of 3,000,000 shares of common stock at an initial price to the public of $6.50 per share, and we received net proceeds of approximately $17.1 million. Our underwriters exercised their option to purchase 450,000 additional shares of common stock to cover over-allotments on November 18, 2014, pursuant to which we received net proceeds of approximately $2.7 million. Also, in conjunction with the IPO, we issued warrants to the underwriters for the purchase of 90,000 shares of common stock, which were exercisable during the period between November 10, 2015 and November 10, 2018 at an exercise price of $8.125 per share. These warrants expired on November 10, 2018.
On November 25, 2015, we closed on our follow-on public offering of 2,272,727 shares of common stock, at a price to the public of $5.50 per share. We granted the underwriters a 45-day option to purchase up to 340,909 additional shares of common stock to cover over-allotments, if any. On December 30, 2015, our underwriters exercised their over-allotment option to purchase an additional 340,909 shares of common stock at a price of $5.50 per share. After giving effect to the over-allotment exercise, the total number of shares offered and sold in our follow-on public offering increased to 2,613,636 shares. With the over-allotment option exercise, we received aggregate net proceeds of approximately $13.0 million.
We deliver convenient, appointment-free chiropractic adjustments in an inviting, open bay environment at prices that are approximately 62% lower than the average industry cost for comparable procedures offered by traditional chiropractors, according to 2018 industry data from Chiropractic Economics. In support of our mission to offer quality, affordable and convenient care to our patients, our clinics offer a variety of customizable membership and wellness treatment plans which provide additional value pricing even as compared with our single-visit pricing schedules. These flexible plans are designed to attract patients and encourage repeat visits and routine usage as part of an overall health and wellness program.
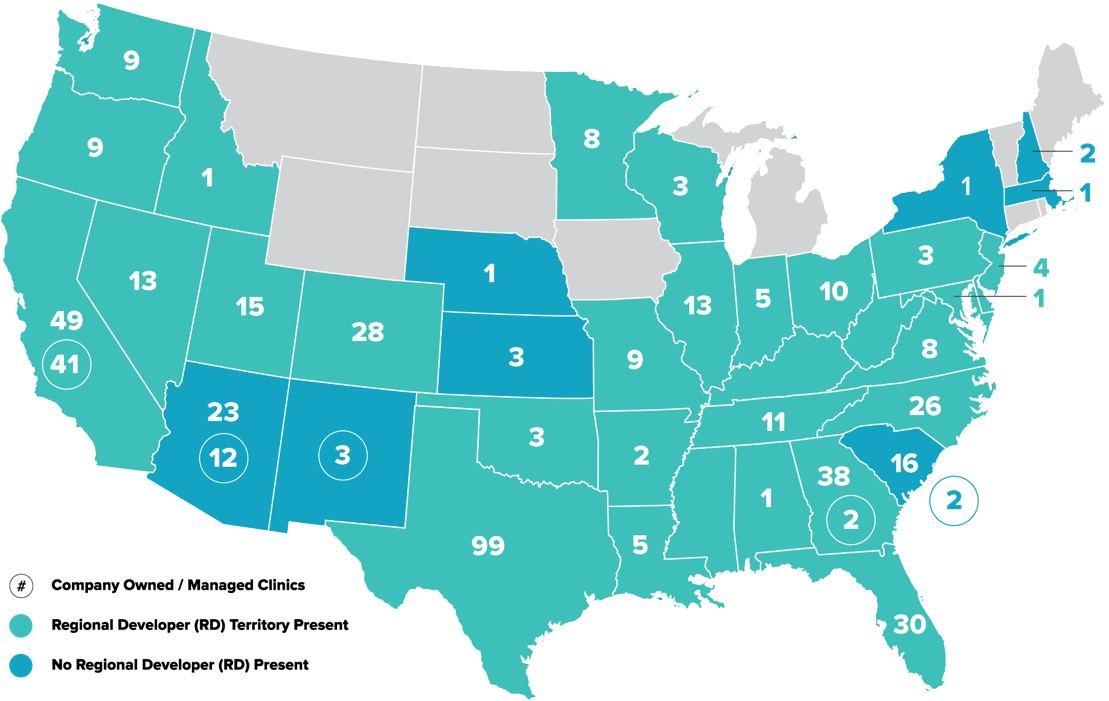
As of December 31, 2019, we had 513 franchised or company-owned or managed clinics in operation in 34 states. The map below shows the states in which we or our franchisees operate clinics and the number of clinics open in each state as of December 31, 2019.
Our retail locations have been selected to be visible, accessible and convenient. We offer a welcoming, consumer-friendly experience that attempts to redefine the chiropractic doctor/patient relationship. Our clinics are open longer hours than many of our competitors, including weekend days, and our patients do not need appointments. We accept cash or major credit cards in return for our services. We do not accept insurance and do not provide Medicare covered services. We believe that our approach, especially our commitment to affordable pricing and our ready service delivery model, will attract existing consumers of chiropractic services and will also appeal to the growing market of consumers who seek alternative or non-invasive wellness care, but have not yet tried chiropractic. According to our patient survey conducted in early 2019 by WestGroup Research, 26% of our new patients had never tried chiropractic care before they came to The Joint. This represents an increase from 22% of patients new to chiropractic in the same survey conducted in 2017, 21% in 2016 and 16% in 2013, demonstrating our continued impact on the chiropractic market and offering validation to our thesis that we are actually expanding the overall market for chiropractic.
Our patients arrive at our clinics without appointments at times convenient to their schedules. Once a patient has joined our system and is returning for treatment, they simply swipe their membership card at a card reader at the reception desk to announce their arrival. The patient is then escorted to our open adjustment area, where they are required to remove only their outerwear to receive their adjustment. Each patient’s records are digitally updated for retrieval in our proprietary data storage system by our chiropractors in compliance with all applicable medical records security and privacy regulations. The adjustment process, administered by a licensed chiropractor, takes approximately 15 - 20 minutes on average for a new patient and 5 - 7 minute on average for a returning patient.
Our consumer-focused service model targets the non-acute treatment market, which is part of the $15 billion chiropractic services market, according to IBIS market research report in February 2019. As our model does not focus on the treatment of severe or acute injury, we do not provide expensive and invasive diagnostic tools such as MRIs and X-rays. Instead we refer those with severe or acute symptoms to alternate healthcare providers, including traditional chiropractors.
Our Industry
Chiropractic care is widely accepted among individuals with a variety of medical conditions, particularly back pain. It is estimated that chiropractors treat more than 52 million Americans (adults and children) annually. A 2018 Gallup report commissioned by Palmer College of Chiropractic shows that among all U.S. adults, including those who did not have neck or back pain, 16% went to a chiropractor in the last 12 months. These numbers represent a marked increase over the 2012 National Health Interview Survey that measured chiropractic use at 8% of the population. According to the American Chiropractic Association, 80% of Americans experience back pain at least once in their lifetime. According to the same 2018 Gallup report commissioned by the Palmer College of Chiropractic, eight in 10 adults in the United States (80%) prefer to see a health care professional who is an expert in spine-related conditions for neck or back pain care instead of a general medicine professional who treats a variety of conditions (15%).
Chiropractic care is increasingly recognized as an effective treatment for pain and potentially for a variety of other conditions. The American College of Physicians (ACP) now recommends non-drug therapy such as spinal manipulation as a first line of treatment for patients with chronic low-back pain. The ACP states that treatments such as spinal manipulation are shown to improve symptoms with little risk of harm. The National Center for Complementary & Alternative Medicine of the National Institutes of Health has stated that spinal manipulation appears to benefit some people with low-back pain and also may be helpful for headaches, neck pain, upper- and lower-extremity joint conditions and whiplash-associated disorders. The Mayo Clinic has recognized chiropractic as safe when performed by trained and licensed chiropractors, and the Cleveland Clinic has stated that chiropractors are established members of the mainstream medical team.
The chiropractic industry in the United States is large and highly fragmented. The Bureau of Labor Statistics estimates that $90 billion is spent on back pain each year in the U.S. According to a report issued by IBIS World Chiropractors Market Research in February 2019, expenditures for chiropractic services in the U.S. are $15 billion annually. The United States Bureau of Labor Statistics expects employment in chiropractic to grow faster than the average for all occupations. Some of the factors that the Bureau of Labor Statistics identified as driving this growth are healthcare cost pressures, an aging population requiring more health care and technological advances, all of which are expected to increasingly shift services from inpatient facilities and hospitals to outpatient settings. We believe that the demand for our chiropractic services will continue to grow as a result of several additional drivers, such as the growing recognition of the benefits of regular maintenance therapy coupled with an increasing awareness of the convenience of our service and of our pricing at a significant discount to the cost of traditional chiropractic adjustments and, in most cases, at or below the level of insurance co-payment amounts.
Today, most chiropractic services are provided by sole practitioners, generally in medical office settings. The chiropractic industry differs from the broader healthcare services industry in that it is more heavily consumer-driven, market-responsive and price sensitive, in large measure a result of many treatment options falling outside the bounds of traditional insurance reimbursable services and fee schedules. According to a First Research report from June 2019, the top 50 companies delivering chiropractic services in the United States generated less than 10% of all industry revenue. We believe these characteristics are evidence of an underserved market with potential consumer demand that is favorable for an efficient, low-cost, consumer-oriented provider.
Most chiropractic practices are set up to accept and to process insurance-based reimbursement. While chiropractors typically accept cash payment in addition to insurance, Medicare and Medicaid, they continue to incur overhead expenses associated with maintaining the capability to process third-party reimbursement. We believe that most chiropractors who use this third-party reimbursement model would find it economically difficult to discount the prices they charge for their services to levels comparable with our pricing.
Accordingly, we believe these and certain other trends favor our business model. Among these are:
•People, most notably Millennials – the largest portion of our patient base – have increasingly active lifestyles and are living longer, requiring more medical, maintenance and preventative support;
•People are increasingly open to alternative, non-pharmacological types of care;
•Utilization of more conveniently situated, local-sited urgent-care or “mini-care” alternatives to primary care is increasing; and
•Popularity of health clubs, massage and other non-drug, non-invasive wellness maintenance providers is growing.
Our Competitive Strengths
We believe the following competitive strengths have contributed to our initial success and will position us for future growth:
Retail, consumer-driven approach. To support our consumer-focused model, we use strong, recognizable retail approaches to stimulate brand-awareness and attract patients to our clinics. We intend to continue to drive awareness of our brand by locating clinics mainly at retail centers and convenience points, displaying prominent signage and employing consistent, proven and targeted marketing tools. We offer our patients the flexibility to visit our clinics without an appointment and receive prompt attention. Additionally, most of our clinics offer extended hours of operation, including weekends, which is not typical among our competitors.
We attracted an average of 1,224 new patients per clinic (for all clinics open for the full twelve months of 2019) during the year ended December 31, 2019, as compared to the 2019 chiropractic industry average of 332 new patients per year for traditional insurance-based non-multidisciplinary or integrated practices, according to a 2019 Chiropractic Economics survey.
Quality, Empathetic Service. Across our system we have a community of approximately 1,500 fully licensed chiropractic doctors, who performed approximately 7.7 million adjustments last year alone. Our doctors provide personal and intuitive patient care focused on pain relief and ongoing wellness to promote healthy, active lifestyles. We provide our doctors one-on-one training, as well as ongoing coaching and mentoring. Our doctors continually refine their skills, as our clinics see an average of 326 patient visits per week (for clinics open for the full twelve months of 2019), as compared to the 2019 chiropractic industry average of 123 patients per week for non-multidisciplinary or integrated practices, according to a 2019 Chiropractic Economics survey. Our service offerings encourage consumer trial, repeat visits and sustainable patient relationships.
By limiting the administrative burdens of insurance processing, our model helps chiropractors focus on patient service. We believe the time our chiropractors save by not having to perform administrative duties related to insurance reimbursement allows more time to see more patients, establish and reinforce chiropractor/patient relationships, and educate patients on the benefits of chiropractic maintenance therapy.
Our approach has made us an attractive alternative for chiropractic doctors who want to spend more time treating patients than they typically do in traditional practices, which are burdened with greater overhead, personnel and administrative expense. We believe that our model helps us to recruit chiropractors who want to focus their practice principally on patient care.
Accessibility. We believe that our strongest competitive advantages are our convenience and affordability. By focusing on non-acute care in an open-bay environment and by not participating in insurance or Medicare reimbursement, we are able to offer a much less expensive alternative to traditional chiropractic services. We can do this because our clinics do not have the expenses of performing certain diagnostic procedures and processing reimbursement claims. Our model allows us to pass these savings on to our patients. According to Chiropractic Economics in 2018, the average fee for a chiropractic treatment involving spinal manipulation in a cash-based practice in the United States is approximately $77. By comparison, our average fee as of December 31, 2019 was approximately $29, approximately 62% lower than the industry average price.
We believe our pricing and service offering structure helps us to generate higher usage. The following table sets forth our average price per adjustment as of December 31, 2019 for patients who pay by single adjustment plans, multiple adjustment packages, and multiple adjustment membership plans. Our price per adjustment as of December 31, 2019 averaged approximately $29 across all three groups.
| | | | | | | | | | | | | | | | | |
| The Joint Service Offering | | | | |
| Single Visit | | Package(s) | | Membership(s) |
| Price per adjustment | $ | 39 | | | $21—$33 | | | $17—$20 | |
Proven track record of opening clinics and growing revenue at the clinic level. We have grown our clinic revenue base consistently. From January 2012 through December 31, 2019, we have increased average monthly sales across our clinics from $0.4 million to $18.4 million. During this period, we increased the number of clinics in operation from 33 to 513.
We continue to be encouraged by the ability of individual clinics to generate growth. While there is significant variation in results in our system, and the results of our top-performing clinics are not representative of our system overall, we believe it is worth noting that in January 2012, the highest-performing clinic in our system was a franchise clinic which had monthly sales of approximately $45,000, and in December 2019, the highest performing clinic in our system was a franchise clinic which had monthly sales of approximately $141,000.
Strong and proven management team. Our strategic vision is directed by our president and chief executive officer, Peter D. Holt, who has more than 30 years of experience in domestic and international franchising, franchise development and operations. Under his direction, we have confirmed our commitment to the continued strengthening of operations, the continued cultivation and management of our franchise community, as well as a strong commitment to future clinic development both domestically and internationally. Mr. Holt was most recently president and chief executive officer of Tasti-D-Lite. He has also served as chief operating officer of 24seven Vending (U.S), where he directed its franchise system in the U.S., and as executive vice president of development for Mail Boxes Etc. and vice president of international for I Can’t Believe It’s Yogurt and Java Coast Fine Coffees. Mr. Holt directs a team of dedicated leaders who are focused on executing our business plan and implementing our growth strategy.
Mr. Holt has assembled a strong management team including Jake Singleton as chief financial officer. In addition to valuable institutional memory from his over three years serving as our corporate controller, Mr. Singleton has financial and accounting experience from his time with the public accounting firm Ernst & Young LLP.
In 2016, Eric Simon joined as vice president of franchise sales and development with over 20 years of experience in all aspects of franchising, most recently as director of franchise development for AAMCO Transmissions. Mr. Simon spent five years as a franchisee and area developer with Extreme Pita and previously spent 10 years with Mail Boxes Etc. in franchise sales roles.
In 2017, Jorge Armenteros joined as vice president of operations bringing with him more than 40 years of franchise operations and leadership experience. For 10 years prior to joining the team, Mr. Armenteros was the executive senior vice president of franchise operations and corporate development for Campero USA, a fast food restaurant chain. Prior to that, he was founder and chief executive officer of Tri-Brands Management Group, which operated franchised Dunkin’ Donuts, Baskin Robbins and Togo restaurants, and was vice president of operations at Dunkin’ Brands. His career also includes a period as a multi-unit franchisee of Dunkin’ Donuts.
Amy Karroum was promoted to vice president of human resources in 2017, having joined us in 2015. Prior to working at The Joint, Ms. Karroum was director of human resources for Thermo Fluids, an oil recycling company, and before that, she spent five years in homebuilding with both Taylor Morrison and Pulte Homes.
In 2018, Jason Greenwood joined our management team as vice president of marketing. Mr. Greenwood spent the last 10 years at Peter Piper Pizza in progressively responsible roles, most recently as chief marketing officer. Prior to that, he was a multi-unit franchisee for Robeks Juice.
Also in 2018, Manjula Sriram joined our management team as vice president of information technology. Prior to working at The Joint, Ms. Sriram spent the last three years at Early Warning Services in progressively responsible roles, most recently as director of customer implementation and support. Prior to that, she performed various senior technical and project management roles at Vail Systems, Inc, US Foods, Walgreens and United Airlines.
We believe that our management team’s experience and demonstrated success in building and operating a robust franchise system will be a key driver of our growth and will position us well for achieving our long-term strategy.
Our Growth Strategy
Our goal is not only to capture a significant share of the existing market but also to expand the market for chiropractic care. We are accomplishing this through the rapid geographic expansion of our affordable franchising program and the opportunistic addition of company-owned or managed clinics. Accordingly, our long-term growth tactics include:
•the continued growth of system sales and royalty income;
•accelerating the opening of clinics already in development;
•the sale of additional franchises;
•the sale of additional regional developer protected territories;
•increasing the capability and capacity of our existing regional developer network;
•improving operational margins and leveraging infrastructure;
•the opportunistic acquisition of existing franchises – referred to as “buybacks”; and
•the development of company-owned clinics – referred to as “greenfields” – in clustered geographies.
Our analysis of patient records data from 513 clinics suggests that the United States market alone can support at least 1,800 of our clinics.
Continued growth of system sales.
System wide comparable same-store sales growth, or “Comp Sales,” for 2019 was 25%, reflecting the growing acceptance of The Joint business model. Comp Sales refers to the amount of sales a clinic generates in the most recent accounting period, compared to the amount of sales it generated in a similar period in the past. Comp Sales include the sales from both company-owned or managed clinics and franchised clinics that in each case have been open at least 13 full months and exclude any clinics that have closed. We believe that the experience we have gained in developing and refining management systems, operating standards, training materials and marketing and customer acquisition activities has contributed to our system’s revenue growth. In addition, we believe that increasing awareness of our brand has contributed to revenue growth, particularly in markets where the number and density of our clinics has made cooperative and mass media advertising attractive. We believe that our ability to leverage aggregated and general media digital advertising and search tools will continue to grow as the number and density of our clinics increases.
Selling additional franchises.
We will continue to sell franchises. We believe that to secure leadership in our industry and to maximize our opportunities in our markets, it is important to gain brand equity and consumer awareness as rapidly as possible, consistent with a disciplined approach to opening clinics. We believe that continued sales of franchises in selected markets is the most effective way to drive brand awareness in the short term. As discussed below, consistent with our longer-term strategy, we will continue to open or acquire company-owned or managed clinics, and we believe that a growth strategy that includes both franchised and company-owned or managed clinics has advantages over either approach by itself.
Selling additional Regional Developer rights.
We believe that we can achieve scale faster by using a regional developer model, which is employed by many successful franchisors. We sell a regional developer the rights to open a minimum number of clinics in a defined territory. They in turn help us to identify and qualify potential new franchisees in that territory and assist us in providing field training, clinic openings and ongoing support. In return, we share part of the initial franchise fee and pay the regional developer 3% of the 7% ongoing royalties we collect from the franchisees in their protected territory. In 2018, we sold the rights to an additional four regional developer territories for a combined minimum development commitment of 111 clinics over the lifetime of their regional developer agreements. In 2019, we sold the rights to 1 additional regional developer territory for a combined minimum development commitment of 40 clinics over a ten-year period. In 2019, regional developers were responsible for 89% of the
126 franchise license sales for the year. This growth reflects the power of the regional developer program to accelerate the number of clinics opening across the country.
Opening clinics in development.
In addition to our 513 operating clinics, as of December 31, 2019, we have granted franchises, either directly or with our regional developers' support, for an additional 170 clinics that we believe will be developed in the future and executed 34 letters-of-intent for future clinic licenses. We will continue to support our franchisees and regional developers to open these clinics and to achieve sustainable performance as rapidly as possible.
Continue to improve margins and leverage infrastructure.
We believe our corporate infrastructure can support a clinic base greater than our existing footprint. As we continue to grow, we expect to drive greater efficiencies across our operations, development and marketing programs and further leverage our technology and existing support infrastructure. We believe we will be able to control corporate costs over time to enhance margins as general and administrative expenses grow at a slower rate than our clinic base and sales. As a percentage of revenue, general and administrative expenses during the year ended December 31, 2019 and 2018 were 63% and 69%, respectively, reflecting improved leverage of our operating model. At the clinic level, we expect to drive margins and labor efficiencies through continued sales growth and consistently applied operating standards as our clinic base matures and the average number of patient visits increases. In addition, we will consider introducing selected and complementary branded products such as nutraceuticals or dietary supplements and related additional services.
Acquiring existing franchises.
We believe that we can accelerate the development of, and revenue generation from, company-owned or managed clinics through the further selective acquisition of existing franchised clinics. We will continue to pursue the acquisition of existing franchised clinics that meet our criteria for demographics, site attractiveness, proximity to other clinics and additional suitability factors. Following the completion of the IPO through December 31, 2019, we acquired 43 existing franchises, subsequently closed three, and continue to operate 40 of them as company-owned or managed clinics.
Development of company-owned or managed clinics.
We acquired our first company-owned or managed clinic on December 31, 2014. In the first full calendar quarter after that acquisition, total revenue from company-owned or managed clinics was $0.4 million, growing to approximately $7.6 million in the quarter ended December 31, 2019. Total revenue from our 60 company-owned or managed clinics was approximately $25.8 million for the year ended December 31, 2019 as compared to $19.5 million from 48 company-owned or managed clinics for the year ended December 31, 2018. Through December 31, 2019, revenue from company-owned or managed clinics consisted of revenue earned from 40 franchised clinics that we acquired, as well as 20 clinics that we developed.
Consistent with our strategies discussed above, we intend to continue to target geographic clusters where we are able to increase efficiencies through a consolidated real estate penetration strategy, leverage cooperative advertisement and marketing, and attain general corporate and administrative operating efficiencies. We also believe that the development timeline and point of break-even for company-owned or managed clinics will be shortened as compared to our previous greenfield openings and that our revenue from company-owned or managed clinics will ultimately exceed revenue that would be generated through royalty income from a franchise-only system.
Regulatory Environment
HIPAA
In an effort to further combat healthcare fraud and protect patient confidentiality, Congress included several anti-fraud measures in the Health Insurance Portability and Accountability Act of 1996 (HIPAA). HIPAA created a source of funding for fraud control to coordinate federal, state and local healthcare law enforcement programs, conduct investigations, provide guidance to the healthcare industry concerning fraudulent healthcare practices, and establish a national data bank to receive and report final adverse actions. HIPAA also criminalized certain forms of healthcare fraud against all public and private payors. Additionally, HIPAA mandated the adoption of standards regarding the exchange of healthcare information in an effort to ensure the privacy and security of electronic patient information. Sanctions for failing to comply with HIPAA include criminal penalties and civil sanctions. In February 2009, the American Recovery and Reinvestment Act of 2009 (ARRA) was enacted. Title XIII of ARRA, the Health Information Technology for Economic and Clinical Health Act (HITECH), included substantial Medicare and Medicaid incentives for providers to adopt electronic health records (“EHR”) and grants for the development of
health information exchange (“HIE”) systems. Recognizing that HIE and EHR systems would not be implemented unless the public could be assured that the privacy and security of patient information in such systems is protected, HITECH also significantly expanded the scope of the privacy and security requirements under HIPAA. Most notable were mandatory breach notification requirements and a heightened enforcement scheme that included increased penalties, expanded to apply to business associates as well as to covered entities. In addition to HIPAA, a number of states have adopted laws and/or regulations applicable in the use and disclosure of individually identifiable health information that can be more stringent than comparable provisions under HIPAA and HITECH.
We believe that our operations substantially comply with applicable standards for privacy and security of protected healthcare information, but such ongoing compliance involves significant time, effort and expense.
State regulations on corporate practice of chiropractic.
In states that regulate the “corporate practice of chiropractic,” chiropractic services are provided solely by legal entities organized under state laws as professional corporations, or PCs or their equivalents. Each of the PCs is wholly owned by one or more licensed chiropractors and employs or contracts with chiropractors in one or more offices. We do not own any capital stock of (or have any other ownership interest in) any such PC. We and our franchisees that are not owned by chiropractors enter into management services agreements with PCs to provide the PCs on an exclusive basis with all non-clinical administrative services needed by the chiropractic practice.
In February 2020, the State of Washington Chiropractic Quality Assurance Commission delivered notices that it was investigating complaints made against three chiropractors who own clinics, or are (or were) employed by clinics, in Washington for which our franchisees provide management services. The notices contained allegations of fee-splitting, specifically questioning a provision in our Franchise Disclosure Document providing for the payment of royalty fees based on revenue derived from the furnishing of chiropractic care. The notices requested that the chiropractors provide responses to a number of questions posed by the commission, as well as documentation describing the fee structure and related matters. The notices appear to question our business model. The investigations initiated by the commission have just begun, and we are not yet aware of the full extent of the commission’s concerns. As these investigations proceed, we will assist the chiropractors in working toward a resolution.
In February 2019, a bill was introduced in the Arkansas state legislature prohibiting the ownership and management of a chiropractic corporation by a non-chiropractor. The bill was drafted by the Arkansas State Board of Chiropractic Examiners. This bill has since been withdrawn. While it is questionable whether the prohibition would have been applicable to our business model in Arkansas, the bill could have been interpreted to challenge that model if it had passed in its proposed form. We have no assurance that another bill posing a similar or greater challenge to our business model will not be introduced in the future. Previously, in 2015, the Arkansas Board had questioned whether our business model might violate Arkansas law in its response to an inquiry we made on behalf of one of our franchisees. While the Arkansas Board did not thereafter pursue the matter of a possible violation, it might choose to do so at any time in the future.
In February 2019, the North Carolina Board of Chiropractic Examiners delivered notices alleging certain violations to sixteen chiropractors working for clinics in North Carolina for which our franchisees provide management services. We retained legal counsel in this matter, and a preliminary hearing was conducted on February 21, 2019. The North Carolina Board issued its findings to each of the individual chiropractors, which generally included an overall finding that probable cause existed to show that the chiropractors violated one or more of the North Carolina Board’s rules. The findings each also proposed an Informal Settlement Agreement in lieu of proceeding to a full hearing before the North Carolina Board. On April 22, 2019, each of the chiropractors, through their attorneys, delivered to the North Carolina Board notices refuting the North Carolina Board’s findings and seeking revisions to the Settlement Agreement. The North Carolina Board replied with certain counter proposals, and all chiropractors have since accepted the terms. While the allegations consisted primarily of quality of care and advertising issues, it is possible that the actions of the North Carolina Board arose out of concerns related to our business model, and if so, we have no assurance that the North Carolina Board will not pursue other claims against the chiropractors in the future.
In November 2018, the Oregon Board of Chiropractic Examiners adopted changes to its rules to prohibit a chiropractor from owning or operating a chiropractic practice as a surrogate for a non-chiropractor. As in the case of the proposed Arkansas bill, the rules changes could be interpreted to challenge our business model in Oregon, although it is similarly questionable whether the prohibition would be applicable. Previously in 2018, the Oregon Board exchanged correspondence with us requesting clarification of our business model and separately with one of our franchisees alleging a violation of the rules against the corporate practice of chiropractic. We provided the requested clarification in March 2018, and the Oregon Board has not
taken any additional action to date. After a further exchange of correspondence with the franchisee, the Oregon Board notified the franchisee in August 2018 that the case was closed.
In November 2015, the California Board of Chiropractic Examiners commenced an administrative proceeding to which we were not a party, in which it claimed that the doctor who owns the PC that we manage in southern California violated California’s prohibition on the corporate practice of chiropractic, among other claims, because our management of the clinics operated by his PC involved the exercise of control over certain clinical aspects of his practice. The California Board of Chiropractic Examiners subsequently dismissed those claims in congruence with findings of the overseeing administrative judge.
In June 2015, the New York Attorney General announced that it had entered into an Assurance of Discontinuance with a provider of business services to independently owned dental practices in New York, pursuant to which the provider paid a substantial fine and agreed to change its business and branding practices. The Assurance of Discontinuance settled claims, among others, that the provider improperly made business decisions impacting clinical matters and engaged in fee-splitting with dental practices. While it has not done so to date, the New York Attorney General could similarly choose to challenge our contractual relationships with our affiliated PCs in New York.
The Kansas Healing Arts Board, in response to a third-party complaint about one of our franchisees, sent a letter to the franchisee in February 2015 questioning whether the franchise business model might violate Kansas law regarding the unauthorized practice of chiropractic care. At the time, we and the franchisee had several communications with the Kansas Board with respect to modifying the management agreement to address its concerns. While we have had no further communications with the Board since that time, we have also received no assurance that changes to the agreement satisfied its concerns.
While the effect of the Arkansas bill if passed, the Oregon rules changes, and the proceedings in Washington, North Carolina, California, New York and Kansas may be that our business practices in those states are under stricter scrutiny than elsewhere, we believe we are in substantial compliance with all applicable laws relating to the corporate practice of chiropractic.
Please see the risk factor in Item 1A beginning with the phrase “Our management services agreements” for a more detailed discussion of state regulations on the “corporate practice of chiropractic” as they relate to our business model.
Regulation relating to franchising
We are subject to the rules and regulations of the Federal Trade Commission and various state laws regulating the offer and sale of franchises. The Federal Trade Commission and various state laws require that we furnish a Franchise Disclosure Document or FDD containing certain information to prospective franchisees, and a number of states require registration of the FDD at least annually with state authorities. Included in the information required to be disclosed in our FDD is our business experience, material litigation, all fees due to us from franchisees, a franchisee’s estimated initial investment, restrictions on sources of products and services we impose on franchisees, development and operating obligations of franchisees, whether we provide financing to franchisees, our training and support obligations and other terms and conditions of our franchise agreement. We are operating under exemptions from registration in several states based on our qualifications for exemption as set forth in those states’ laws. Substantive state laws regulating the franchisor-franchisee relationship presently exist in many states. We believe that our FDD and franchising procedures comply in all material respects with both the Federal Trade Commission guidelines and all applicable state laws regulating franchising in those states in which we have offered franchises. As of December 31, 2019, we were registered to sell franchises in every state (where registrations are required); and could sell franchises in all 50 states.
Other federal, state and local regulation
We are subject to varied federal regulations affecting the operation of our business. We are subject to the U.S. Fair Labor Standards Act, the U.S. Immigration Reform and Control Act of 1986, the Occupational Safety and Health Act and various other federal and state laws governing such matters as minimum wage requirements, overtime, fringe benefits, workplace safety and other working conditions and citizenship requirements. A significant number of our clinic service personnel are paid at rates related to the applicable minimum wage and increases in the minimum wage could increase our labor costs. We are continuing to assess the impact of federal health care legislation on our health care benefit costs. Many of our smaller franchisees qualify for exemption from the requirement to either provide health insurance benefits or pay a penalty to the IRS if not provided because of their small number of employees. The imposition of any requirement that we or our franchisees provide
health insurance benefits to our or their employees that are more extensive than the health insurance benefits that we currently provide to our employees or that franchisees may or may not provide, or the imposition of additional employer paid employment taxes on income earned by our employees, could have an adverse effect on our results of operations and financial position. Our distributors and suppliers also may be affected by higher minimum wage and benefit standards, which could result in higher costs for goods and services supplied to us.
A final rule issued in January 2020 by the Department of Labor (or “DOL”) narrowed the meaning of “joint employer” under the Fair Labor Standards Act (FLSA), the federal law that sets minimum wage and overtime standards. The final DOL rule focuses on a potential joint employer’s actual direct or indirect control over an employee, including whether the potential joint employer supervises an employee’s conditions of employment to a substantial degree, and identifies certain business models, including franchising, that do not in themselves make joint employer status more or less likely. The final DOL rule reverses the more expansive definition of “joint employer,” adopted in a July 2014 National Labor Relations Board (or “NLRB”) action holding that McDonald’s Corporation, as a joint employer, could be held jointly liable for labor and wage violations by its franchisees. Note that McDonald’s Corporation was not ultimately required to admit liability or joint-employer status, following a December 2019 NLRB action which instructed an administrative law judge to approve a settlement agreement resolving complaints against McDonald’s Corporation and a number of its franchisees. The affected labor union and a union-backed group have indicated that they will appeal the NLRB action. We believe that the final DOL rule will be more favorable to us by making it less likely that we will be held accountable for the actions of our franchisees. However, it is important to note that the final DOL rule only affects the joint employer standard applicable under the FLSA. The test for joint employer status may be different under other federal and state laws, although rules similarly narrowing the interpretation of “joint employer” are reportedly being worked on by the Equal Employment Opportunity Commission pertaining to workplace discrimination and have been adopted by the NLRB pertaining to collective bargaining, discussed below.
A final rule issued by the NLRB in February 2020, consistent with the DOL’s rule, applies a narrow interpretation of “joint employer” in the collective bargaining context, in which a unionized joint employer has or shares an obligation to collectively bargain over those employment terms it controls or jointly controls. In a manner similar to the DOL’s rulemaking with respect to the FLSA, the final NLRB rule reverses the more expansive definition of “joint employer” applied in the NLRB’s 2015 decision in the case of Browning-Ferris Industries. In that case, Browning-Ferris was deemed to be a joint employer obligated to negotiate with the Teamsters union over workers supplied by a contract staffing firm within one of its recycling plants. The final NLRB rule provides that, in order to be a joint employer, among other things, a business must possess and exercise substantial direct and immediate control over one or more essential conditions of employment of another employer’s employees. We believe that the final NLRB rule will be more favorable to us by making it less likely that employees of our franchisees can organize, bargain collectively, and require us to participate in collective bargaining with those employees. It is expected that the final DOL rule will be challenged in court, given that it conflicts with a December 2018 decision of the U.S. Court of Appeals for the D.C. Circuit, which partially upheld the 2015 Browning-Ferris expansive definition of “joint employer.”
California adopted Assembly Bill 5, or AB-5, which took effect on January 1, 2020. This legislation codifies the standard established in California case law for determining whether workers should be classified as employees or independent contractors, with a strict test that puts the burden of proof on employers to establish that workers are not employees. The law is aimed at the so-called “gig economy” and is not a franchise-specific law, nor does it address the concept of joint employer liability. However, a significant concern exists in the franchise industry that an expansive interpretation of AB-5 could be used to hold franchisors jointly liable for the labor law violations of its franchisees, and it remains uncertain as to how the joint employer issue will ultimately be resolved. The International Franchise Association is actively lobbying in California and has been seeking an amendment to AB-5 that provides an exception for “legitimate franchisors and franchisees.” Please see the risk factor in Item 1A beginning with the phrase “Past decisions by the United States National Labor Relations Board expanding the meaning of ‘joint employer’ and evolving state laws” for a more detailed discussion of the significance of AB-5 in the context of the franchise industry.
We are required to comply with the accessibility standards mandated by the U.S. Americans with Disabilities Act of 1990 and related federal and state statutes, which generally prohibit discrimination in accommodation or employment based on disability. We may, in the future, have to modify our clinics to provide service to or make reasonable accommodations for disabled persons. While these expenses could be material, our current expectation is that any such actions will not require us to expend substantial funds.
We are subject to extensive and varied state and local government regulation affecting the operation of our business, as are our franchisees, including regulations relating to public and occupational health and safety, sanitation, fire prevention and franchise operation. Each franchised clinic is subject to licensing and regulation by a number of governmental authorities, which include zoning, health, safety, sanitation, environmental, building and fire agencies in the jurisdiction in which the clinic
is located. We require our franchisees to operate in accordance with standards and procedures designed to comply with applicable codes and regulations. However, our or our franchisees’ inability to obtain or retain health or other licenses would adversely affect operations at the impacted clinic or clinics. Although we have not experienced and do not anticipate any significant difficulties, delays or failures in obtaining required licenses, permits or approvals, any such problem could delay or prevent the opening of, or adversely impact the viability of, a particular clinic. In addition, in order to develop and construct our clinics, we need to comply with applicable zoning and land use regulations. Federal and state regulations have not had a material effect on our operations to date, but more stringent and varied requirements of local governmental bodies with respect to zoning and land use could delay or even prevent construction and increase development costs of new clinics.
Competition
The chiropractic industry is highly fragmented. According to First Research’s 2019 report, the top 50 providers of chiropractic services in the United States generate less than 10% of industry revenue. Our competitors include approximately 40,000 independent chiropractic offices currently open throughout the United States, according to a 2019 Kentley Insights market research report, as well as certain multi-unit operators. We may also face competition from traditional medical practices, outpatient clinics, physical therapists, med-spas, massage therapists and sellers of devices intended for home use to address back and joint discomfort. Our three largest multi-unit competitors are HealthSource Chiropractic, ChiroOne Wellness Centers, and 100% Chiropractic, all of which are insurance-based models.
We have identified five competitors who are attempting to duplicate our cash-only, low cost, appointment-free model. Based on publicly available information, these competitors each operate fewer than 12 clinics as franchises. We anticipate that other direct competitors will join our industry as our visibility, reputation and perceived advantages become more widely known. We believe our first mover advantage, proprietary operations systems, and strong unit level economics will continue to accelerate our growth even with the spawning of additional competition.
Employees
As of December 31, 2019, we had 150 employees on a full-time basis. None of our employees are members of unions or participate in other collective bargaining arrangements.
Facilities
We lease the property for our corporate headquarters and all of the properties on which we own or manage clinics. As of December 31, 2019, we leased 65 facilities in which we operate or intend to operate clinics. We are obligated under 2 additional leases for facilities in which we have ceased clinic operations.
Our corporate headquarters are located at 16767 North Perimeter Drive, Suite 110, Scottsdale, Arizona 85260. The term of our lease for this location expires on December 31, 2025. The primary functions performed at our corporate headquarters are finance and accounting, treasury, marketing, operations, human resources, information systems support, and legal.
We are also obligated under non-cancellable leases for the clinics which we own or manage. Our clinics are on average 1,200 square feet. Our clinic leases generally have an initial term of five years, include one to two options to renew for terms of five years, and require us to pay a proportionate share of real estate taxes, insurance, common area maintenance charges and other operating costs.
As of December 31, 2019, our franchisees operated 453 clinics in 33 states. All of our franchise locations are leased.
Intellectual Property
Trademarks, trade names and service marks
“The Joint Chiropractic” is our trademark, registered in December 2016, under registration number 5095943. We have also registered "You're Back, Baby" in July 2019, under registration number 5940161, “Back-Tober” in September 2018, under registration number 5571732, "Relief Recovery Wellness" in February 2018, under registration number 5398367, “Pain Relief Is At Hand” in February 2018, under registration number 5395995, “What Life Does To Your Body, We Undo” in February 2018, under registration number 5396012, “Be Chiro-Practical” in October 2017, under registration number 5313693, “Relief. On so many levels” in December 2015, under registration number 4871809, and “The Joint” in April 2015, under registration number 4723892.
Additional trademarks previously registered include “The Joint… the Chiropractic Place” registered in February 2011, under registration number 3922558. We also registered the words, letters, and stylized form of service mark, “The Joint… the Chiropractic Place” in April 2013 under registration number 4323810.
In Canada, we have applied for the following trademarks: “The Joint” in February 2017 under application number 1825026, “The Joint Chiropractic” in February 2017 under application 1825027, the words, letters, and stylized form of trademark “The Joint Chiropractic,” and “The Joint Chiropractic” in February 2017 under application 1825028.
ITEM 1A. RISK FACTORS
Risks Related to Our Business
New clinics, once opened, may not be profitable, and the increases in average clinic sales and comparable clinic sales that we have experienced in the past may not be indicative of future results.
Our clinics continue to demonstrate increases in comparable clinic sales even as they mature. Our annual Comp Sales for the full year 2019, for clinics that have been open for greater than 48 months, was 19%. However, we cannot assure you that this will continue for our existing clinics or that clinics we open in the future will see similar results. In new markets, the length of time before average sales for new clinics stabilize is less predictable and can be longer than we expect because of our limited knowledge of these markets and consumers’ limited awareness of our brand. New clinics may not be profitable and their sales performance may not follow historical patterns. In addition, our average clinic sales and comparable clinic sales for existing clinics may not increase at the rates achieved over the past several years. Our ability to operate new clinics, especially company-owned or managed clinics, profitably and increase average clinic sales and comparable clinic sales will depend on many factors, some of which are beyond our control, including:
•consumer awareness and understanding of our brand;
•general economic conditions, which can affect clinic traffic, local rent and labor costs and prices we pay for the supplies we use;
•changes in consumer preferences and discretionary spending;
•competition, either from our competitors in the chiropractic industry or our own clinics;
•the identification and availability of attractive sites for new facilities and the anticipated commercial, residential and infrastructure development near our new facilities;
•changes in government regulation; and
•other unanticipated increases in costs, any of which could give rise to delays or cost overruns.
If our new clinics do not perform as planned, our business and future prospects could be harmed. In addition, if we are unable to achieve our expected average clinics sales, our business, financial condition and results of operations could be adversely affected.
Our failure to manage our growth effectively could harm our business and operating results.
Our growth plan includes a significant number of new clinics, focused currently on franchised clinics, and the measured and opportunistic addition of company-owned or managed clinics. Our existing clinic management systems, administrative staff, financial and management controls and information systems may be inadequate to support our planned expansion. Those demands on our infrastructure and resources may also adversely affect our ability to manage our existing clinics. Managing our growth effectively will require us to continue to enhance these systems, procedures and controls and to hire, train and retain managers and team members. We may not respond quickly enough to the changing demands that our expansion will impose on our management, clinic teams and existing infrastructure which could harm our business, financial condition and results of operations. We are currently in the process of replacing and upgrading our management information systems, and we cannot provide assurances that we will accomplish this without delays, difficulties or service interruptions.
Our long-term strategy involves opening new, company-owned or managed clinics, and is subject to many unpredictable factors.
One component of our long-term growth strategy is to open new company-owned or managed clinics and to operate those clinics on a profitable basis. As of December 31, 2019, we owned or managed 60 clinics. Previously, we suspended the development of new company-owned or managed clinics from July 2016 through the first quarter of 2018 in order to stabilize our corporate clinic portfolio. We believe we have accomplished that goal, and we have resumed development of such clinics in 2019 and will continue to do so in 2020. We may not be able to open new company-owned or managed clinics as quickly as planned. In the past, we have experienced delays in opening some franchised and company-owned or managed clinics, for various reasons, including construction permitting, landlord responsiveness, and municipal approvals. Such delays could affect future clinic openings. Delays or failures in opening new clinics could materially and adversely affect our growth strategy and our business, financial condition and results of operations. As we operate more clinics, our rate of expansion relative to the size of our clinic base will eventually decline.
In addition, we face challenges locating and securing suitable new clinic sites in our target markets. Competition for those sites is intense, and other retail concepts that compete for those sites may have unit economic models that permit them to bid more aggressively for those sites than we can. There is no guarantee that a sufficient number of suitable sites will be available in desirable areas or on terms that are acceptable to us in order to achieve our growth plan. Our ability to open new clinics also depends on other factors, including:
•negotiating leases with acceptable terms;
•identifying, hiring and training qualified employees in each local market;
•identifying and entering into management agreements with suitable PCs in certain target markets;
•timely delivery of leased premises to us from our landlords and punctual commencement and completion of construction;
•managing construction and development costs of new clinics, particularly in competitive markets;
•obtaining construction materials and labor at acceptable costs, particularly in urban markets;
•unforeseen engineering or environmental problems with leased premises;
•generating sufficient funds from operations or obtaining acceptable financing to support our future development;
•securing required governmental approvals, permits and licenses (including construction permits and operating licenses) in a timely manner and responding effectively to any changes in local, state or federal laws and regulations that adversely affect our costs or ability to open new clinics; and
•the impact of inclement weather, natural disasters and other calamities.
Our expansion into new markets may be more costly and difficult than we currently anticipate which would result in slower growth than we expect.
Clinics we open in new markets may take longer to reach expected sales and profit levels on a consistent basis and may have higher construction, occupancy, marketing or operating costs than clinics we open in existing markets, thereby affecting our overall profitability. New markets may have competitive conditions, consumer tastes and discretionary spending patterns that are more difficult to predict or satisfy than our existing markets. We may need to make greater investments than we originally planned in advertising and promotional activity in new markets to build brand awareness. We may find it more difficult in new markets to hire, motivate and keep qualified employees who share our vision and culture. We may also incur higher costs from entering new markets, particularly with company-owned clinics if, for example, we hire and assign regional managers to manage comparatively fewer clinics than in more developed markets. For these reasons, both our new franchised clinics and our new company-owned or managed clinics may be less successful than our existing franchised clinics or may achieve target rates of patient visits at a slower rate. If we do not successfully execute our plans to enter new markets, our business, financial condition and results of operations could be materially adversely affected.
Opening new clinics in existing markets may negatively affect revenue at our existing clinics.
The target area of our clinics varies by location and depends on a number of factors, including population density, other available retail services, area demographics and geography. As a result, the opening of a new clinic in or near markets in which
we already have clinics could adversely affect the revenues of those existing clinics. Existing clinics could also make it more difficult to build our patient base for a new clinic in the same market. Our business strategy does not entail opening new clinics that we believe will materially affect revenue at our existing clinics, but we may selectively open new clinics in and around areas of existing clinics that are operating at or near capacity to effectively serve our patients. Revenue “cannibalization” between our clinics may become significant in the future as we continue to expand our operations and could affect our revenue growth, which could, in turn, adversely affect our business, financial condition and results of operations.
Any acquisitions that we make could disrupt our business and harm our financial condition.
From time to time, we may evaluate potential strategic acquisitions of existing franchised clinics to facilitate our growth. We may not be successful in identifying acquisition candidates. In addition, we may not be able to continue the operational success of any franchised clinics we acquire or successfully integrate any businesses that we acquire. We may have potential write-offs of acquired assets and an impairment of any goodwill recorded as a result of acquisitions. Furthermore, the integration of any acquisition may divert management’s time and resources from our core business and disrupt our operations or may result in conflicts with our business. Any acquisition may not be successful, may reduce our cash reserves and may negatively affect our earnings and financial performance. We cannot ensure that any acquisitions we make will not have a material adverse effect on our business, financial condition and results of operations.
Damage to our reputation or our brand in existing or new markets could negatively impact our business, financial condition and results of operations.
We believe we have built our reputation on high quality, empathetic patient care, and we must protect and grow the value of our brand to continue to be successful in the future. Our brand may be diminished if we do not continue to make investments in areas such as marketing and advertising, as well as the day-to-day investments required for facility operations, equipment upgrades and staff training. Any incident, real or perceived, regardless of merit or outcome, that erodes our brand, such as failure to comply with federal, state or local regulations including allegations or perceptions of non-compliance or failure to comply with ethical and operating standards, could significantly reduce the value of our brand, expose us to adverse publicity and damage our overall business and reputation. Further, our brand value could suffer and our business could be adversely affected if patients perceive a reduction in the quality of service or staff.
We may be unable to maintain or improve our operating margins, which could adversely affect our financial condition and ability to grow.
If we are unable to successfully manage our growth, we may not be able to capture the efficiencies and opportunities that we expect from our expansion strategy. If we are not able to capture expected efficiencies of scale, maintain patient volumes, improve our systems and equipment, continue our cost discipline and retain appropriate chiropractors and overall labor levels, our operating margins may stagnate or decline, which could have a material adverse effect on our business, financial condition and results of operations and adversely affect the price of our common stock.
We have experienced net losses and may not achieve or sustain profitability in the future.
We have experienced periods of net losses in the past and while we have recently achieved profitability, our revenue may not grow and we may not maintain profitability in the future. Our ability to maintain profitability will be affected by the other risks and uncertainties described in this section and in Management’s Discussion and Analysis. If we are not able to sustain or increase profitability, our business will be materially adversely affected and the price of our common stock may decline.
Our marketing programs may not be successful.
We incur costs and expend other resources in our marketing efforts to attract and retain patients. Our marketing activities are principally focused on increasing brand awareness and driving patient volumes. As we open new facilities, we undertake aggressive marketing campaigns to increase community awareness about our growing presence. We plan to utilize targeted marketing efforts within local neighborhoods through channels such as radio, digital media, community sponsorships and events, and a robust online/social media presence. These initiatives may not be successful, resulting in expenses incurred without the benefit of higher revenue. Our ability to market our services may be restricted or limited by federal or state law.
We will be subject to all of the risks associated with leasing space subject to long-term non-cancelable leases for clinics that we intend to operate.
We do not own, and we do not intend to own, any of the real property where our company-owned or managed clinics operate. We expect the spaces for the company-owned or managed clinics we intend to open in the future will be leased. We anticipate that our leases generally will have an initial term of five or ten years and generally can be extended only in five-year increments (at increased rates). We expect that all of our leases will require a fixed annual rent, although some may require the payment of additional rent if clinic sales exceed a negotiated amount. We expect that our leases will typically be net leases, which require us to pay all of the costs of insurance, taxes, maintenance and utilities, and that these leases will not be cancellable by us. If a future company-owned clinic is not profitable, resulting in its closure, we may nonetheless be committed to perform our obligations under the applicable lease including, among other things, paying the base rent for the balance of the lease term. In addition, we may fail to negotiate renewals as each of our leases expires, either on commercially acceptable terms or at all, which could cause us to pay increased occupancy costs or to close clinics in desirable locations. These potential increases in occupancy costs and the cost of closing company-owned or managed clinics could materially adversely affect our business, financial condition or results of operations. We have settled disputes over future rent with landlords at all of the fourteen clinics that we either closed or never opened.
Our increased reliance on sources of revenue other than from franchise and regional developer licenses exposes us to risks including the loss of revenue and reduction of working capital.
From the commencement of our operations until we began to acquire or open company-owned or managed clinics, we relied exclusively on the sale of franchises and regional developer licenses as sources of revenue until the franchises we sold began to generate royalty revenues. As our portfolio of company-owned or managed clinics matures, we have placed less reliance on these franchise sources of revenue. As we develop further company-owned or managed clinics, we will be required to use our working capital to operate our business. If the opening of our company-owned or managed clinics is delayed or if the cost of developing company-owned or managed clinics exceeds our expectations, we may experience insufficient working capital to fully implement our development plans, and our business, financial condition and results of operations could be adversely affected.
Our potential need to raise additional capital to accomplish our objectives of expanding into new markets and selectively developing company-owned or managed clinics exposes us to risks including limiting our ability to develop or acquire clinics and limiting our financial flexibility.
We resumed the selective development and acquisition of company-owned or managed clinics in the first quarter of 2018. If we do not have sufficient cash resources, our ability to develop and acquire clinics could be limited unless we are able to obtain additional capital through future debt or equity financing. Using cash to finance development and acquisition of clinics could limit our financial flexibility by reducing cash available for operating purposes. Using debt financing could result in lenders imposing financial covenants that limit our operations and financial flexibility. Using equity financing may result in dilution of ownership interests of our existing stockholders. We may also use common stock as consideration for the future acquisition of clinics. If our common stock does not maintain a sufficient market value or if prospective acquisition candidates are unwilling to accept our common stock as part of the consideration for the sale of their clinics or businesses, we may be required to use more of our cash resources or greater debt financing to complete these acquisitions.
Our dependence on the success of our franchisees exposes us to risks including the loss of royalty revenue and harm to our brand.
A substantial portion of our revenues comes from royalties generated by our franchised clinics. We anticipate that franchise royalties will represent a substantial part of our revenues in the future. As of December 31, 2019, we had franchisees operating or managing 453 clinics. Accordingly, we are reliant on the performance of our franchisees in successfully opening and operating their clinics and paying royalties to us on a timely basis. Our franchise system subjects us to a number of risks as described in the next four risk factors, any one of which could impact our ability to collect royalty payments from our franchisees, may harm the goodwill associated with our brand and may materially adversely affect our business and results of operations.
Our franchisees are independent operators over whom we have limited control.
Franchisees are independent operators, and their employees are not our employees. Accordingly, their actions are outside of our control. Although we have developed criteria to evaluate and screen prospective franchisees, we cannot be certain that our franchisees will have the business acumen or financial resources necessary to operate successful franchises in their approved locations, and state franchise laws may limit our ability to terminate or modify these franchise agreements. Moreover, despite our training, support and monitoring, franchisees may not successfully operate clinics in a manner consistent with our standards and requirements, or may not hire and adequately train qualified personnel. The failure of our franchisees to operate their
franchises successfully and the actions taken by their employees could have a material adverse effect on our reputation, our brand and our ability to attract prospective franchisees, and on our business, financial condition and results of operations.
We are subject to the risk that our franchise agreements may be terminated or not renewed.
Each franchise agreement is subject to termination by us as the franchisor in the event of a default, generally after expiration of applicable cure periods, although under certain circumstances a franchise agreement may be terminated by us upon notice without an opportunity to cure. The default provisions under the franchise agreements are drafted broadly and include, among other things, any failure to meet operating standards and actions that may threaten our intellectual property. In addition, each franchise agreement has an expiration date. Upon the expiration of the franchise agreement, we or the franchisee may, or may not, elect to renew the franchise agreement. If the franchise agreement is renewed, the franchisee will receive a new franchise agreement for an additional term. Such option, however, is contingent on the franchisee’s execution of the then-current form of franchise agreement (which may include increased royalty payments, advertising fees and other costs) and the payment of a renewal fee. If a franchisee is unable or unwilling to satisfy any of the foregoing conditions, we may elect not to renew the expiring franchise agreement, in which event the franchise agreement will terminate upon expiration of its term. The termination or non-renewal of a franchise agreement could result in the reduction of royalty payments we receive.
Our franchisees may not meet timetables for opening their clinics, which could reduce the royalties we receive.
Our franchise agreements specify a timetable for opening the clinic. Failure by our franchisees to open their clinics within the specified time limit would result in the reduction of royalty payments we would have otherwise received and could result in the termination of the franchise agreement. As of December 31, 2019, we had 170 active licenses which we believe to be developable and an additional 34 letters-of-intent for future clinic licenses. Of these, 35 have not met their development requirements within the time periods specified in their franchise agreements.
Our franchisees may elect bankruptcy protection and deprive us of income.
The bankruptcy of a franchisee could negatively impact our ability to collect payments due under such franchisee’s franchise agreement. In a franchisee bankruptcy, the bankruptcy trustee may reject the franchisee’s franchise agreement pursuant to Section 365 under the United States Bankruptcy Code, in which case we would no longer receive royalty payments from the franchisee.
Our regional developers are independent operators over whom we have limited control.
Our regional developers are independent operators. Accordingly, their actions are outside of our control. We depend upon our regional developers to sell a minimum number of franchises within their territory and to assist the purchasers of those franchises to develop and operate their clinics. The failure by regional developers to sell the specified minimum number of franchises within the time limits set forth in their regional developer license agreements would reduce the franchise fees we would otherwise receive, delay the payment of royalties to us and result in a potential event of default under the regional developer license agreement. Of our total of twenty one regional developers as of December 31, 2019, five have not met their minimum franchise sales requirements within the time periods specified in their regional developer agreements.
Our ability to operate effectively could be impaired if we fail to attract and retain our executive officers.
Our success depends, in part, upon the continuing contributions of our executive officers and key employees at the management level. Although we have employment letter agreements with renewing one-year terms with certain of our key executive officers, there is no guarantee that they will not leave. The loss of the services of any of our executive officers or the failure to attract other executive officers could have a material adverse effect on our business or our business prospects. If we lose the services of any of our key employees at the operating or regional level, we may not be able to replace them with similarly qualified personnel, which could harm our business.
A lack of qualified employees will significantly hinder our growth plans and adversely affect our results of operations.
As we grow, our ability to increase productivity and profitability will be limited by our ability to employ, train, and retain skilled personnel. There can be no assurance that we will be able to maintain an adequate skilled labor force necessary to operate efficiently, that our labor expenses will not increase as a result of a shortage in the supply of skilled personnel or that we will not have to curtail our planned internal growth as a result of labor shortages.
We may not be able to successfully recruit and retain qualified chiropractors.
Our success depends upon our continuing ability to recruit and retain qualified chiropractors. In the event we are unable to attract a sufficient number of qualified chiropractors, our growth rate may suffer.
Our clinics and chiropractors compete for patients in a highly competitive environment that may make it more difficult to increase patient volumes and revenues.
The business of providing chiropractic services is highly competitive in each of the markets in which our clinics operate. The primary bases of such competition are quality of care and reputation, price of services, marketing and advertising strategy and implementation, convenience, traffic flow and visibility of office locations and hours of operation. Our clinics compete with all other chiropractors in their local market. Many of those chiropractors have established practices and reputations in their markets. Some of these competitors and potential competitors may have financial resources, affiliation models, reputations or management expertise that provide them with competitive advantages over us, which may make it difficult to compete against them. Our three largest multi-unit competitors are HealthSource Chiropractic, which currently operates 166 units; ChiroOne Wellness Centers, which currently operates 58 units domestically; and 100% Chiropractic, which currently operates 35 units. Each of these competitors is currently operating under an insurance-based model. In addition, a number of other chiropractic franchises and chiropractic practices that are attempting to duplicate or follow our business model are currently operating in our markets and in other parts of the country and may enter our existing markets in the future.
Our success is dependent on the chiropractors who control the professional corporations, or PC owners, with whom we enter into management services agreements, and we may have difficulty locating qualified chiropractors to replace PC owners.
In states that regulate the corporate practice of chiropractic, our chiropractic services are provided by legal entities organized under state laws as professional corporations, or PCs and their equivalents. Each PC employs or contracts with chiropractors in one or more offices. Each of the PCs is wholly owned by one or more licensed chiropractors, or medical professionals as state law may require, and we do not own any capital stock of any PC. We and our franchisees that are not owned by chiropractors enter into management services agreements with PCs to provide on an exclusive basis all non-clinical services of the chiropractic practice. The PC owner is critical to the success of a clinic because he or she has control of all clinical aspects of the practice of chiropractic and the provision of chiropractic services. Upon the departure of a PC owner, we may not be able to locate one or more suitably qualified licensed chiropractors to hold the ownership interest in the PC and maintain the success of the departing PC owner.
Major public health concerns, including the outbreak of epidemic or pandemic contagious disease, such as the coronavirus, may adversely affect revenue at our clinics and disrupt financial markets.
In January 2020, the World Health Organization declared that the coronavirus outbreak, which began in China and has since spread to other areas, is a global health emergency. The expected spread of coronavirus in the United States or a similar public health threat, or fear of such an event, may negatively impact the willingness of patients to visit our clinics or the shopping centers in which they are located out of concern over exposure to contagious disease. A prolonged outbreak, resulting in reduced patient traffic and continued disruptions to capital and financial markets, could have a material adverse impact on our business, financial condition, results of operations, and the market price of our stock.
Changes in economic conditions and adverse weather and other unforeseen conditions could materially affect our ability to maintain or increase sales at our clinics or open new clinics.
Our services emphasize maintenance therapy, which is generally not a medical necessity, and should be viewed as a discretionary medical expenditure. The United States in general or the specific markets in which we operate may suffer from depressed economic activity, recessionary economic cycles, higher fuel or energy costs, low consumer confidence, high levels of unemployment, reduced home values, increases in home foreclosures, investment losses, personal bankruptcies, reduced access to credit or other economic factors that may affect consumer discretionary spending. Traffic in our clinics could decline if consumers choose to reduce the amount they spend on non-critical medical procedures. Negative economic conditions might cause consumers to make long-term changes to their discretionary spending behavior, including reducing medical discretionary spending on a permanent basis. In addition, given our geographic concentrations in the West, Southwest and mid-Atlantic regions of the United States, economic conditions in those particular areas of the country could have a disproportionate impact on our overall results of operations, and regional occurrences such as local strikes, terrorist attacks, increases in energy prices, adverse weather conditions, tornadoes, earthquakes, hurricanes, floods, droughts, fires or other natural or man-made disasters could materially adversely affect our business, financial condition and results of operations. Adverse weather conditions may
also impact customer traffic at our clinics. All of our clinics depend on visibility and walk-in traffic, and the effects of adverse weather may decrease visits to malls in which our clinics are located and negatively impact our revenues. If clinic sales decrease, our profitability could decline as we spread fixed costs across a lower level of sales. Reductions in staff levels, asset impairment charges and potential clinic closures could result from prolonged negative clinic sales, which could materially adversely affect our business, financial condition and results of operations.
Our management services agreements, according to which we provide non-clinical services to affiliated PCs, could be challenged by a state or chiropractor under laws regulating the practice of chiropractic, and some state chiropractic boards have made inquiries concerning our business model.
The laws of every state in which we operate contain restrictions on the practice of chiropractic and control over the provision of chiropractic services. The laws of many states where we operate permit a chiropractor to conduct a chiropractic practice only as an individual, a member of a partnership or an employee of a PC, limited liability company or limited liability partnership. These laws typically prohibit chiropractors from splitting fees with non-chiropractors and prohibit non-chiropractic entities, such as chiropractic management services organizations, from owning or operating chiropractic clinics or engaging in the practice of chiropractic and from employing chiropractors. The specific restrictions against the corporate practice of chiropractic, as well as the interpretation of those restrictions by state regulatory authorities, vary from state to state. However, the restrictions are generally designed to prohibit a non-chiropractic entity from controlling or directing clinical care decision-making, engaging chiropractors to practice chiropractic or sharing professional fees. The form of management agreement that we utilize, and that we recommend to our franchisees that are management service organizations, explicitly prohibits the management service organization from controlling or directing clinical care decisions. However, there can be no assurance that all of our franchisees that are management service organizations will strictly follow the provisions in our recommended form of management agreement. The laws of many states also prohibit chiropractic practitioners from paying any portion of fees received for chiropractic services in consideration for the referral of a patient. Any challenge to our contractual relationships with our affiliated PCs by chiropractors or regulatory authorities could result in a finding that could have a material adverse effect on our operations, such as voiding one or more management services agreements. Moreover, the laws and regulatory environment may change to restrict or limit the enforceability of our management services agreements. We could be prevented from affiliating with chiropractor-owned PCs or providing comprehensive business services to them in one or more states.
In February 2020, the State of Washington Chiropractic Quality Assurance Commission delivered notices that it was investigating complaints made against three chiropractors who own clinics, or are (or were) employed by clinics, in Washington for which our franchisees provide management services. The notices contained allegations of fee-splitting, specifically questioning a provision in our Franchise Disclosure Document providing for the payment of royalty fees based on revenue derived from the furnishing of chiropractic care. The notices requested that the chiropractors provide responses to a number of questions posed by the commission, as well as documentation describing the fee structure and related matters. The allegations pose a threat to our business model, and unless we can resolve the commission’s concerns to its satisfaction, our franchisees may be required to change their service arrangements with clinics, and we may be required to change our business model in the State of Washington.
In February 2019, a bill was introduced in the Arkansas state legislature prohibiting the ownership and management of a chiropractic corporation by a non-chiropractor. The bill was drafted by the Arkansas State Board of Chiropractic Examiners. This bill has since been withdrawn. While it is questionable whether the prohibition would have been applicable to our business model in Arkansas, the bill could have been interpreted to challenge that model if it had passed in its proposed form. We have no assurance that another bill posing a similar or greater challenge to our business model will not be introduced in the future. Previously, in 2015, the Arkansas Board had questioned whether our business model might violate Arkansas law in its response to an inquiry we made on behalf of one of our franchisees. While the Arkansas Board did not thereafter pursue the matter of a possible violation, it might choose to do so at any time in the future.
In February 2019, the North Carolina Board of Chiropractic Examiners delivered notices alleging certain violations to sixteen chiropractors working for clinics in North Carolina for which our franchisees provide management services. We retained legal counsel in this matter, and a preliminary hearing was conducted on February 21, 2019. The North Carolina Board issued its findings to each of the individual chiropractors, which generally included an overall finding that probable cause existed to show that the chiropractors violated one or more of the North Carolina Board’s rules. The findings each also proposed an Informal Settlement Agreement in lieu of proceeding to a full hearing before the North Carolina Board. On April 22, 2019, each of the chiropractors, through their attorneys, delivered to the North Carolina Board notices refuting the North Carolina Board’s findings and seeking revisions to the Settlement Agreement. The North Carolina Board replied with certain counterproposals, and all chiropractors have since accepted the terms. While the allegations consisted primarily of quality of care and advertising issues, it is possible that the actions of the North Carolina Board arose out of concerns related to our
business model, and if so, we have no assurance that the North Carolina Board will not pursue other claims against the chiropractors in the future.
In November 2018, the Oregon Board of Chiropractic Examiners adopted changes to its rules to prohibit a chiropractor from owning or operating a chiropractic practice as a surrogate for a non-chiropractor. As in the case of the proposed Arkansas bill, it is questionable whether this prohibition is applicable to our business model in Oregon; however, depending upon how the amended rules are interpreted, they could similarly pose a threat. Since our franchisees began operating in Oregon, the Oregon Board has made several inquiries with respect to our business model. We have typically satisfied these inquiries by providing a brief response or documentation. In February 2018, the Oregon Board asked us for clarification regarding ownership of our franchise locations operating in Oregon, and we responded with the requested clarification. The Oregon Board has not taken any further action, but we have no assurance that it will not do so in the future or that we have satisfied the Oregon Board’s concerns. One of our franchisees received a letter from the Oregon Board alleging a violation of the rules against the corporate practice of chiropractic, but after a further exchange of correspondence with the franchisee, the Oregon Board notified the franchisee in August 2018 that the case was closed.
In November 2015, the California Board of Chiropractic Examiners commenced an administrative proceeding to which we were not a party, in which it claimed that the doctor who owns the PC that we manage in southern California violated California’s prohibition on the corporate practice of chiropractic, among other claims, because our management of the clinics operated by his PC involved the exercise of control over certain clinical aspects of his practice. The claims were subsequently dismissed congruent with the decision of the administrative law judge who conducted the proceeding; however, we cannot assure you that similar claims will not be made in the future, either against us or our affiliated PCs.
In a June 2015 Assurance of Discontinuance with the New York Attorney General, Aspen Dental Management, a provider of business support services to independently owned dental practices, agreed to settle claims that it improperly made business decisions impacting clinical matters, illegally engaged in fee-splitting with dental practices and required the dental practices to use the “Aspen Dental” trade name in a manner that had the potential to mislead consumers into believing that the “Aspen Dental”- branded offices were under common ownership with the provider. Pursuant to the settlement, Aspen Dental paid a substantial fine and agreed to change its business and branding practices, including changes to its website and marketing materials in order to make clear that the Aspen-branded dental offices were independently owned and operated. While it has not done so to date, we cannot assure you that the New York Attorney General will not similarly choose to challenge our contractual relationships with our affiliated PCs in New York and, in particular, to question whether use of The Joint trademark by our affiliated PCs misleads consumers, causing them to incorrectly conclude that we are the provider of chiropractic treatment.
The Kansas Healing Arts Board, in response to a third-party complaint about one of our franchisees, sent a letter to the franchisee in February 2015 questioning whether the franchise business model might violate Kansas law regarding the unauthorized practice of chiropractic care. At the time, we and the franchisee had several communications with the Kansas Board with respect to modifying the management agreement to address its concerns. While we have had no further communications with the Board since that time, we have also received no assurance that changes to the agreement satisfied its concerns.
Past decisions by the United States National Labor Relations Board expanding the meaning of “joint employer” and evolving state laws mean that we could have liability for employment law violations by our franchisees.
A July 2014 decision by the United States National Labor Relations Board (or NLRB) held that McDonald’s Corporation could be held liable as a “joint employer” for labor and wage violations by its franchisees under the Fair Labor Standards Act (FLSA). After this decision, the NLRB issued a number of complaints against McDonald’s Corporation in connection with these violations. Additionally, an August 2015 decision by the NLRB held that Browning-Ferris Industries was a “joint employer” for purposes of collective bargaining and, thus, obligated to negotiate with the Teamsters union over workers supplied by a contract staffing firm within one of its recycling plants.
Since then, in January 2020, the Department of Labor (or “DOL”) issued a final rule narrowing the meaning of “joint employer” under the FLSA. Furthermore, McDonald’s Corporation in the aforementioned NLRB action was not ultimately required to admit liability or joint-employer status. However, the affected labor union and a union-backed group have indicated that they will appeal the decision, and there may be other legal challenges to the DOL rule. Consistent with the DOL’s rule, the NLRB issued a final rule in February 2020, narrowing the meaning of “joint employer” in the collective bargaining context. As in the case of the DOL rule, it is expected that the final NLRB rule will be challenged in court, given that it conflicts with a
December 2018 decision of the U.S. Court of Appeals for the D.C. Circuit, which partially upheld the 2015 Browning-Ferris expansive definition of “joint employer.”
Should the new DOL rule narrowing the meaning of “joint employer” ultimately be rejected by the courts or replaced by rules returning to a more expansive definition of “joint employer” in a stricter regulatory climate, we could have responsibility for damages, reinstatement, back pay and penalties in connection with labor law violations by our franchisees over whom we have limited control, which could have a material adverse effect on our financial condition and results of operations. Similarly, a rollback of the NLRB rule could make it easier for our franchisees’ employees to organize into unions, require us to participate in collective bargaining with those employees, provide those employees and their union representatives with bargaining power to request that we have our franchisees raise wages, and make it more expensive and less profitable to operate a franchised clinic. Additionally, notwithstanding the narrowing of the meaning of “joint employer” under the FLSA and collective bargaining rules, the test for joint employer status may be different under other federal laws and under state laws.
California adopted Assembly Bill 5, or AB-5, which took effect on January 1, 2020. This legislation codifies the standard established in a California Supreme Court case (Dynamex Operations West v. Superior Court) for determining whether workers should be classified as employees or independent contractors, with a strict test that puts the burden of proof on employers to establish that workers are not employees. The law is aimed at the so-called “gig economy” where workers in many industries, particularly ride-sharing industries, are treated as independent contractors, rather than employees, and lack the protections of wage and hour laws. AB-5 is not a franchise-specific law and does not address joint employer liability; however, a significant concern exists in the franchise industry that an expansive interpretation of AB-5 could be used to hold franchisors jointly liable for the labor law violations of its franchisees. Courts addressing this issue have come to differing conclusions. Two different panels of the U.S. Circuit Court of Appeals for the Ninth Circuit, in applying California law, reached contradictory conclusions, with one panel implicitly concluding that the Dynamex standard was applicable to joint liability claims in the franchise industry and a second panel later concluding in December 2019 that it was not applicable. In February 2020, in reviewing the case decided by the first panel, the California Supreme Court denied requests to consider whether the Dynamex standard applies to joint liability claims. It remains uncertain as to how the joint employer issue will ultimately be resolved.
AB-5 has been the subject of widespread national discussion, and it is possible that other jurisdictions may enact similar laws, which might similarly raise concerns with respect to the expansion of joint liability to the franchise industry. Furthermore, there have been private lawsuits in which parties have alleged that a franchisor and its franchisee “jointly employ” the franchisee’s staff, that the franchisor is responsible for the franchisees’ staff (under theories of apparent agency, ostensible agency, or actual agency), or otherwise.
Evolving labor and employment laws, rules and regulations, and theories of liability could result in expensive litigation and potential claims against us as a franchisor for labor and employment-related and other liabilities that have historically been borne by franchisees. This could negatively impact the franchise business model, which could materially and adversely affect our business, financial condition and results of operations.
We and our affiliated chiropractor-owned PCs are subject to complex laws, rules and regulations, compliance with which may be costly and burdensome.
We, our franchisees and the chiropractor-owned PCs to which we and our franchisees provide management services are subject to extensive federal, state and local laws, rules and regulations, including:
•state regulations on the practice of chiropractic;
•the Health Insurance Portability and Accountability Act of 1996, as amended, and its implementing regulations, or HIPAA, and other federal and state laws governing the collection, dissemination, use, security and confidentiality of patient-identifiable health and financial information;
•federal and state laws and regulations which contain anti-kickback and fee-splitting provisions and restrictions on referrals;
•the federal Fair Debt Collection Practices Act and similar state laws that restrict the methods that we and third-party collection companies may use to contact and seek payment from patients regarding past due accounts; and
•state and federal labor laws, including wage and hour laws.
Many of the above laws, rules and regulations applicable to us, our franchisees and our affiliated PCs are ambiguous, have not been definitively interpreted by courts or regulatory authorities and vary from jurisdiction to jurisdiction. Accordingly, we may not be able to predict how these laws and regulations will be interpreted or applied by courts and regulatory authorities, and some of our activities could be challenged. In addition, we must consistently monitor changes in the laws and regulatory schemes that govern our operations. Although we have tried to structure our business and contractual relationships in
compliance with these laws, rules and regulations in all material respects, if any aspect of our operations were found to violate applicable laws, rules or regulations, we could be subject to significant fines or other penalties, required to cease operations in a particular jurisdiction, prevented from commencing operations in a particular state or otherwise be required to revise the structure of our business or legal arrangements. Our efforts to comply with these laws, rules and regulations may impose significant costs and burdens, and failure to comply with these laws, rules and regulations may result in fines or other charges being imposed on us.
We conduct business in a heavily regulated industry and, if we fail to comply with these laws and government regulations, we could incur penalties or be required to make significant changes to our operations.
The healthcare industry is heavily regulated and closely scrutinized by federal, state and local governments. Comprehensive statutes and regulations govern the manner in which we provide and bill for services, our contractual relationships with our physicians, vendors and customers, our marketing activities and other aspects of our operations. Failure to comply with these laws can result in civil and criminal penalties such as fines, damages, overpayment recoupment, loss of enrollment status or exclusion from government healthcare programs. The risk of our being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by regulatory authorities or the courts, and their provisions are sometimes open to multiple interpretations. Any action against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our managements’ attention from the operation of our business.
Our chiropractors are also subject to ethical guidelines and operating standards of professional and trade associations and private accreditation agencies. Compliance with these guidelines and standards is often required by our contracts with our customers or to maintain our reputation. The laws, regulations and standards governing the provision of healthcare services may change significantly in the future. New or changed healthcare laws, regulations or standards may materially and adversely affect our business. In addition, a review of our business by judicial, law enforcement, regulatory or accreditation authorities could result in a determination that could adversely affect our operations.
Our facilities are subject to extensive federal and state laws and regulations relating to the privacy and security of individually identifiable information.
HIPAA required the United States Department of Health and Human Service, or HHS, to adopt standards to protect the privacy and security of individually identifiable health-related information, or PHI. HHS released final regulations containing privacy standards in December 2000 and published revisions to the final regulations in August 2002. The privacy regulations extensively regulate the use and disclosure of PHI. The regulations also provide patients with significant rights related to understanding and controlling how their health information is used or disclosed. The security regulations require healthcare providers to implement administrative, physical and technical practices to protect the security of individually identifiable health information that is maintained or transmitted electronically. The Health Information Technology for Economic and Clinical Health Act, or HITECH, which was signed into law in February of 2009, enhanced the privacy, security and enforcement provisions of HIPAA by, among other things, extending HIPAA’s privacy and security standards to “business associates,” which, like us, are independent contractors or agents of covered entities (such as the chiropractic PCs and other healthcare providers) that create, receive, maintain, or transmit PHI in connection with providing a service for or on behalf of a covered entity. HITECH also established security breach notification requirements, created a mechanism for enforcement of HIPAA by state attorneys general, and increased penalties for HIPAA violations. Violations of HIPAA or HITECH could result in civil or criminal penalties. In addition to HIPAA, there are numerous federal and state laws and regulations addressing patient and consumer privacy concerns, including unauthorized access or theft of personal information. State statutes and regulations vary from state to state. Lawsuits, including class actions and action by state attorneys general, directed at companies that have experienced a privacy or security breach also can occur. We have established policies and procedures in an effort to ensure compliance with these privacy related requirements. However, if there is a breach, we may be subject to various penalties and damages and may be required to incur costs to mitigate the impact of the breach on affected individuals.
We are subject to the data privacy, security and breach notification requirements of HIPAA and other data privacy and security laws, and the failure to comply with these rules, or allegations that we have failed to do so, can result in civil or criminal sanctions.
HIPAA required the United States Department of Health and Human Service, or HHS, to adopt standards to protect the privacy and security of certain health-related information. The HIPAA privacy regulations contain detailed requirements concerning the use and disclosure of individually identifiable health information and the grant of certain rights to patients with respect to such information by “covered entities.” As a provider of healthcare who conducts certain electronic transactions, each of our facilities is considered a covered entity under HIPAA. We have taken actions to comply with the HIPAA privacy
regulations and believe that we are in compliance with those regulations. Oversight of HIPAA compliance involves significant time, effort and expense.
In addition to the privacy requirements, HIPAA covered entities must implement certain administrative, physical and technical security standards to protect the integrity, confidentiality and availability of certain electronic health-related information received, maintained or transmitted by covered entities or their business associates. We have taken actions in an effort to be in compliance with these security regulations and believe that we are in compliance, however, a security incident that bypasses our information security systems causing an information security breach, loss of protected health information or other data subject to privacy laws or a material disruption of our operational systems could result in a material adverse impact on our business, along with fines. Ongoing implementation and oversight of these security measures involves significant time, effort and expense.
The Health Information Technology for Economic and Clinical Health Act, or HITECH, as implemented in part by an omnibus final rule published in the Federal Register on January 25, 2013, further requires that patients be notified of any unauthorized acquisition, access, use, or disclosure of their unsecured protected health information, or PHI, that compromises the privacy or security of such information. HHS has established the presumption that all unauthorized uses or disclosures of unsecured protected health information constitute breaches unless the covered entity or business associate establishes that there is a low probability the information has been compromised. HITECH and implementing regulations specify that such notifications must be made without unreasonable delay and in no case later than 60 calendar days after discovery of the breach. If a breach affects 500 patients or more, it must be reported immediately to HHS, which will post the name of the breaching entity on its public website. Breaches affecting 500 patients or more in the same state or jurisdiction must also be reported to the local media. If a breach involves fewer than 500 people, the covered entity must record it in a log and notify HHS of such breaches at least annually. These breach notification requirements apply not only to unauthorized disclosures of unsecured PHI to outside third parties, but also to unauthorized internal access to or use of such PHI.
HITECH significantly expanded the scope of the privacy and security requirements under HIPAA and increased penalties for violations. The amount of penalty that may be assessed depends, in part, upon the culpability of the applicable covered entity or business associate in committing the violation. Some penalties for certain violations that were not due to “willful neglect” may be waived by the Secretary of HHS in whole or in part, to the extent that the payment of the penalty would be excessive relative to the violation. HITECH also authorized state attorneys general to file suit on behalf of residents of their states. Applicable courts may award damages, costs and attorneys’ fees related to violations of HIPAA in such cases. HITECH also mandates that the Secretary of HHS conduct periodic compliance audits of a cross-section of HIPAA covered entities and business associates. Every covered entity and business associate is subject to being audited, regardless of the entity’s compliance record.
States may impose more protective privacy restrictions in laws related to health information and may afford individuals a private right of action with respect to the violation of such laws. Both state and federal laws are subject to modification or enhancement of privacy protection at any time. We are subject to any federal or state privacy-related laws that are more restrictive than the privacy regulations issued under HIPAA. These statutes vary and could impose additional requirements on us and more severe penalties for disclosures of health information. If we fail to comply with HIPAA or similar state laws, including laws addressing data confidentiality, security or breach notification, we could incur substantial monetary penalties and our reputation could be damaged.
In addition, states may also impose restrictions related to the confidentiality of personal information that is not considered “protected health information” under HIPAA. Such information may include certain identifying information and financial information of our patients. Theses state laws may impose additional notification requirements in the event of a breach of such personal information. Failure to comply with such data confidentiality, security and breach notification laws may result in substantial monetary penalties.
Our business model depends on proprietary and third-party management information systems that we use to, among other things, track financial and operating performance of our clinics, and any failure to successfully design and maintain these systems or implement new systems could materially harm our operations.
We depend on integrated management information systems, some of which are provided by third parties, and standardized procedures for operational and financial information, as well as for patient records and our billing operations. We are currently replacing and upgrading our management information systems. We may experience unanticipated delays, complications, data breaches or expenses in replacing, upgrading, implementing, integrating, and operating our systems. Our management information systems regularly require modifications, improvements or replacements that may require both substantial expenditures as well as interruptions in operations. Our ability to implement these systems is subject to the availability of
skilled information technology specialists to assist us in creating, implementing and supporting these systems. Our failure to successfully design, implement and maintain all of our systems could have a material adverse effect on our business, financial condition and results of operations.
If we fail to properly maintain the integrity of our data or to strategically implement, upgrade or consolidate existing information systems, our reputation and business could be materially adversely affected.
We increasingly use electronic means to interact with our customers and collect, maintain and store individually identifiable information, including, but not limited to, personal financial information and health-related information. Despite the security measures we have in place to ensure compliance with applicable laws and rules, our facilities and systems, and those of our third-party service providers, may be vulnerable to security breaches, acts of cyber terrorism, vandalism or theft, computer viruses, misplaced or lost data, programming and/or human errors or other similar events. Additionally, the collection, maintenance, use, disclosure and disposal of individually identifiable data by our businesses are regulated at the federal and state levels as well as by certain financial industry groups, such as the Payment Card Industry organization. Federal, state and financial industry groups may also consider from time to time new privacy and security requirements that may apply to our businesses. Compliance with evolving privacy and security laws, requirements, and regulations may result in cost increases due to necessary systems changes, new limitations or constraints on our business models and the development of new administrative processes. They also may impose further restrictions on our collection, disclosure and use of individually identifiable information that is housed in one or more of our databases. Noncompliance with privacy laws, financial industry group requirements or a security breach involving the misappropriation, loss or other unauthorized disclosure of personal, sensitive and/or confidential information, whether by us or by one of our vendors, could have material adverse effects on our business, operations, reputation and financial condition, including decreased revenue; material fines and penalties; increased financial processing fees; compensatory, statutory, punitive or other damages; adverse actions against our licenses to do business; and injunctive relief whether by court or consent order.
If our security systems are breached, we may face civil liability and public perception of our security measures could be diminished, either of which would negatively affect our ability to attract and retain patients.
Techniques used to gain unauthorized access to corporate data systems are constantly evolving, and we may be unable to anticipate or prevent unauthorized access to data pertaining to our patients, including credit card and debit card information and other personally identifiable information. Our systems, which are supported by our own systems and those of third-party vendors, are vulnerable to computer malware, trojans, viruses, worms, break-ins, phishing attacks, denial-of-service attacks, attempts to access our servers in an unauthorized manner, or other attacks on and disruptions of our and third-party vendor computer systems, any of which could lead to system interruptions, delays, or shutdowns, causing loss of critical data or the unauthorized access to personally identifiable information. If an actual or perceived breach of security occurs on our systems or a vendor’s systems, we may face civil liability and reputational damage, either of which would negatively affect our ability to attract and retain patients. We also would be required to expend significant resources to mitigate the breach of security and to address related matters.
We may not be able to effectively control the unauthorized actions of third parties who may have access to the patient data we collect. Any failure, or perceived failure, by us to maintain the security of data relating to our patients and employees, and to comply with our posted privacy policy, laws and regulations, rules of self-regulatory organizations, industry standards and contractual provisions to which we may be bound, could result in the loss of confidence in us, or result in actions against us by governmental entities or others, all of which could result in litigation and financial losses, and could potentially cause us to lose patients, revenue and employees.
We are subject to a number of risks related to credit card and debit card payments we accept.
We accept payments through credit and debit card transactions. For credit and debit card payments, we pay interchange and other fees, which may increase over time. An increase in those fees would require us to either increase the prices we charge for our services, which could cause us to lose patients and revenue, or absorb an increase in our operating expenses, either of which could harm our operating results.
If we or any of our processing vendors have problems with our billing software, or the billing software malfunctions, it could have an adverse effect on patient satisfaction and could cause one or more of the major credit card companies to disallow our continued use of their payment products. In addition, if our billing software fails to work properly, and as a result, we do not automatically process monthly membership fees to our patients’ credit cards on a timely basis or at all, or there are issues with financial insolvency of our third-party vendors or other unanticipated problems or events, we could lose revenue, which would harm our operating results.
We are also subject to payment card association operating rules, certification requirements and rules governing electronic funds transfers, which could change or be reinterpreted to make it more difficult for us to comply. We are not currently accredited against, and in compliance with, the Payment Card Industry Data Security Standard, or PCI DSS, the payment card industry’s security standard for companies that collect, store or transmit certain data regarding credit and debit cards, credit and debit card holders and credit and debit card transactions. Once compliant, there is no guarantee that we will maintain PCI DSS compliance. Our failure to comply fully with PCI DSS in the future could violate payment card association operating rules, federal and state laws and regulations and the terms of our contracts with payment processors and merchant banks. Such failure to comply fully also could subject us to fines, penalties, damages and civil liability and could result in the suspension or loss of our ability to accept credit and debit card payments. Further, there is no guarantee that PCI DSS compliance will prevent illegal or improper use of our payment systems or the theft, loss, or misuse of data pertaining to credit and debit cards, credit and debit card holders and credit and debit card transactions.
If we fail to adequately control fraudulent credit card transactions, we may face civil liability, diminished public perception of our security measures and significantly higher credit card-related costs, each of which could adversely affect our business, financial condition and results of operations. If we are unable to maintain our chargeback or refund rates at acceptable levels, credit and debit card companies may increase our transaction fees, impose monthly fines until resolved or terminate their relationships with us. Any increases in our credit and debit card fees could adversely affect our results of operations, particularly if we elect not to raise our rates for our service to offset the increase. The termination of our ability to process payments on any major credit or debit card would significantly impair our ability to operate our business.
We, along with our affiliated PCs and their chiropractors, are subject to malpractice and other similar claims and may be unable to obtain or maintain adequate insurance against these claims.
The provision of chiropractic services by chiropractors entails an inherent risk of potential malpractice and other similar claims. While we do not have responsibility for compliance by affiliated PCs and their chiropractors with regulatory and other requirements directly applicable to chiropractors, claims, suits or complaints relating to services provided at the offices of our franchisees or affiliated PCs may be asserted against us. As we develop company-owned or managed clinics, our exposure to malpractice claims will increase. We have experienced a number of malpractice claims since our founding in March, 2010, which we have defended or are vigorously defending and do not expect their outcome to have a material adverse effect on our business, financial condition or results of operations. The assertion or outcome of these claims could result in higher administrative and legal expenses, including settlement costs or litigation damages. Our current minimum professional liability insurance coverage required for our franchisees, affiliated PCs and company-owned clinics is $1.0 million per occurrence and $3.0 million in annual aggregate. In addition, we have a corporate business owner’s policy with coverage of $2.0 million per occurrence and $4.0 million in annual aggregate. If we are unable to obtain adequate insurance or if there is an increase in the future cost of insurance to us and the chiropractors who provide chiropractic services or an increase in the amount we have to self-insure, there may be a material adverse effect on our business and financial results.
We could be party to litigation that could adversely affect us by distracting management, increasing our expenses or subjecting us to material monetary damages and other remedies.
In addition to malpractice claims, we are also subject to a variety of other claims arising in the ordinary course of our business, including personal injury claims, contract claims and claims alleging violations of federal and state law regarding workplace and employment matters, equal opportunity, harassment, discrimination and similar matters, and we could become subject to class action or other lawsuits related to these or different matters in the future. Regardless of whether any claims against us are valid, or whether we are ultimately held liable, claims may be expensive to defend and may divert time and money away from our operations and hurt our performance. A judgment in excess of our insurance coverage for any claims could materially and adversely affect our financial condition and results of operations. Any adverse publicity resulting from these allegations may also materially and adversely affect our reputation or prospects, which in turn could materially adversely affect our business, financial condition and results of operations.
We are subject to the risk that our current insurance may not provide adequate levels of coverage against claims.
Our current insurance policies may not be adequate to protect us from liabilities that we incur in our business. Additionally, in the future, our insurance premiums may increase, and we may not be able to obtain similar levels of insurance on reasonable terms, or at all. Any substantial inadequacy of, or inability to obtain insurance coverage could materially adversely affect our business, financial condition and results of operations.
Furthermore, there are types of losses we may incur that cannot be insured against or that we believe are not economically reasonable to insure. Such losses could have a material adverse effect on our business and results of operations. Failure to
obtain and maintain adequate directors’ and officers’ insurance would likely adversely affect our ability to attract and retain qualified officers and directors.
Events or rumors relating to our brand names or our ability to defend successfully against intellectual property infringement claims by third parties could significantly impact our business.
Recognition of our brand names, including “THE JOINT CHIROPRACTIC”, and the association of those brands with quality, convenient and inexpensive chiropractic maintenance care, are an integral part of our business. The occurrence of any events or rumors that cause patients to no longer associate the brands with quality, convenient and inexpensive chiropractic maintenance care may materially adversely affect the value of the brand names and demand for chiropractic services at our franchisees or their affiliated PCs.
Our ability to compete effectively depends in part upon our intellectual property rights, including but not limited to our trademarks. Our use of contractual provisions, confidentiality procedures and agreements, and trademark, copyright, unfair competition, trade secret and other laws to protect our intellectual property rights may not be adequate. Litigation may be necessary to enforce our intellectual property rights, or to defend against claims by third parties that the conduct of our businesses or our use of intellectual property infringes upon such third party’s intellectual property rights. Any intellectual property litigation or claims brought against us, whether or not meritorious, could result in substantial costs and diversion of our resources, and there can be no assurances that favorable final outcomes will be obtained in all cases. Our business, financial condition or results of operations could be adversely affected as a result.
We present Adjusted EBITDA as a supplemental measure to help us describe our operating performance. Adjusted EBITDA is a non-GAAP financial measure commonly used in our industry and should not be construed as an alternative to net income or as a better indicator of operating performance.
Adjusted EBITDA consists of net income before interest, income taxes, depreciation and amortization, acquisition related expenses, stock-based compensation expense, bargain purchase gain, and loss on disposition or impairment. We present Adjusted EBITDA as a supplemental measure to help us describe our operating performance. Adjusted EBITDA is a non-GAAP financial measure commonly used in our industry and should not be construed as an alternative to net income (as determined in accordance with generally accepted accounting principles in the United States, or GAAP) or as a better indicator of operating performance. You should not consider Adjusted EBITDA as a substitute for operating profit, as an indicator of our operating performance or as an alternative to cash flows from operating activities as a measure of liquidity. We may calculate Adjusted EBITDA differently from other companies.
In addition, in the future we may incur expenses similar to those excluded when calculating Adjusted EBITDA. Our presentation of these measures should not be construed as an inference that our future results will be unaffected by unusual or non-recurring items. Our computation of Adjusted EBITDA may not be comparable to other similarly titled measures computed by other companies, because not all companies calculate Adjusted EBITDA in the same manner.
Our management does not consider Adjusted EBITDA in isolation or as an alternative to financial measures determined in accordance with GAAP. The principal limitation of Adjusted EBITDA is that it excludes significant expenses and income that are required by GAAP to be recorded in our financial statements. Some of these limitations are: (i) Adjusted EBITDA does not reflect our cash expenditures, or future requirements, for capital expenditures or contractual commitments; (ii) Adjusted EBITDA does not reflect changes in, or cash requirements for, our working capital needs; (iii) Adjusted EBITDA does not reflect the interest expense, or the cash requirements necessary to service interest or principal payments on our debts, and although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future; (iv) Adjusted EBITDA does not reflect any cash requirements for such replacements; (v) Adjusted EBITDA does not reflect the bargain purchase gain, which represents the excess of the fair value of net assets acquired over the purchase consideration; and (vi) Adjusted EBITDA does not reflect the loss on disposition or impairment, which represents the impairment of assets as of the reporting date. We do not consider these to be indicative of our ongoing operations.
The requirements of being a public company, including compliance with the reporting requirements of the Exchange Act and the requirements of the Sarbanes-Oxley Act, may strain our resources, increase our costs and distract management, and we may be unable to comply with these requirements in a timely or cost-effective manner.
As a public company with listed equity securities, we need to comply with certain laws, regulations and requirements, including corporate governance provisions of the Sarbanes-Oxley Act, related regulations of the SEC, and the requirements of The Nasdaq Stock Market LLC. Complying with these statutes, regulations and requirements occupies a significant amount of time of our Board of Directors and management and has significantly increased our costs and expenses. We will continue to:
•institute more comprehensive corporate governance and compliance functions;
•design, establish, evaluate and maintain a system of internal control over financial reporting in compliance with the requirements of Section 404(a) of the Sarbanes-Oxley Act and the related rules and regulations of the SEC and the Public Company Accounting Oversight Board;
•comply with rules promulgated by The Nasdaq Stock Market LLC;
•prepare and distribute periodic public reports in compliance with our obligations under the federal securities laws;
•establish new internal policies, such as those relating to disclosure controls and procedures and insider trading; and
•involve and retain outside counsel and accountants in the above activities.
Risks Related to Our Public Offerings and Listing of Our Common Stock on the NASDAQ Capital Market
Our stock price could be volatile and could decline.
The price at which our common stock will trade could be extremely volatile and may fluctuate substantially due to the following factors, some of which are beyond our control:
•variations in our operating results;
•variations between our actual operating results and the expectations of securities analysts, investors and the financial community;
•announcements of developments affecting our business or expansion plans by us or others; and
•regulations, conditions, and trends in the chiropractic industry.
As a result of these and other factors, investors in our common stock may not be able to resell their shares at or above their purchase price.
In the past, securities class action litigation often has been instituted against companies following periods of volatility in the market price of their securities. This type of litigation, if directed at us, could result in substantial costs and a diversion of management’s attention and resources.
Provisions of Delaware law could discourage a takeover that stockholders may consider favorable.
As a Delaware corporation, we have elected to be subject to the Delaware anti-takeover provisions contained in Section 203 of the Delaware General Corporation Law. Under Delaware law, a corporation may not engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other things, the Board of Directors has approved the transaction. Our Board of Directors could rely on this provision to prevent or delay an acquisition of us.
Future sales of our common stock may depress our stock price and our share price may decline due to the large number of shares eligible for future sale or exchange.
Sales of substantial amounts of our common stock in the public market by our officers, directors or significant shareholders may adversely affect the market price of our common stock. Shares issued upon the exercise of outstanding options may be sold in the public market. Such sales could create the perception to the public of difficulties or problems with our business. As a result, these sales might make it more difficult for us to sell securities in the future at a time and price that we deem necessary or appropriate.
The market price of our common stock could decline as a result of sales of a large number of shares of common stock in the market or the perception that such sales could occur. These sales, or the possibility that these sales may occur, might also make it more difficult for us to sell equity securities in the future at a time and at a price that we deem appropriate. As of December 31, 2019, we had 13,882,932 outstanding shares of common stock and are authorized to sell up to 20,000,000 shares of common stock. The trading volume of shares of our common stock averaged 151,527 shares per day during the year ended
December 31, 2019. Accordingly, sales of even small amounts of shares of our common stock by existing stockholders may drive down the trading price of our common stock.
If securities analysts do not publish research or reports about our business or if they downgrade our company or our sector, the price of our common stock could decline.
The trading market for our common stock depends in part on the research and reports that industry or financial analysts publish about us or our business. We do not influence or control the reporting of these analysts. If one or more of the analysts who cover us downgrade or provide a negative outlook on our company or our industry, or the stock of any of our competitors, the price of our common stock could decline. If one or more of these analysts ceases coverage of our company, we could lose visibility in the market, which in turn could cause the price of our common stock to decline.
Our actual results may differ from forecasts.
It is difficult to accurately forecast our revenues, operating expenses and results, and operating data. The inability by us or the financial community to accurately forecast our operating results could cause our net income in a given quarter to be less than expected or our net losses in a given quarter to be greater than expected, which could cause a decline in the trading price of our common stock. We base our current and forecasted expense and cash expenditure levels on our operating plans and estimates of future revenues, which are dependent on the growth of the number of patients and the demand for our services. As a result, we may be unable to make accurate financial forecasts or to adjust our spending in a timely manner to compensate for any unexpected shortfalls in revenues. We believe that these difficulties in forecasting are even greater for financial analysts that may publish their own estimates of our financial results.
We do not intend to pay dividends. You will not receive funds without selling shares, and you may lose the entire amount of your investment.
We have never declared or paid any cash dividends on our capital stock and do not intend to pay dividends in the foreseeable future. We intend to invest our future earnings, if any, to fund our growth. We cannot assure you that you will receive a positive return on your investment when you subsequently sell your shares or that you will not lose the entire amount of your investment.
Claims for indemnification by our directors and officers may reduce our available funds to satisfy successful third-party claims against us and may reduce the amount of money available to us.
Our amended and restated certificate of incorporation and bylaws provide that we will indemnify our directors and officers, in each case to the fullest extent permitted by Delaware law. In addition, we have entered and expect to continue to enter into agreements to indemnify our directors, executive officers and other employees as determined by our Board of Directors. Under the terms of such indemnification agreements, we are required to indemnify each of our directors and officers, to the fullest extent permitted by the laws of the state of Delaware, if the basis of the indemnitee’s involvement was by reason of the fact that the indemnitee is or was a director or officer of the Company or any of its subsidiaries or was serving at the Company’s request in an official capacity for another entity. We must indemnify our officers and directors against all reasonable fees, expenses, charges and other costs of any type or nature whatsoever, including any and all expenses and obligations paid or incurred in connection with investigating, defending, being a witness in, participating in (including on appeal), or preparing to defend, be a witness or participate in any completed, actual, pending or threatened action, suit, claim or proceeding, whether civil, criminal, administrative or investigative, or establishing or enforcing a right to indemnification under the indemnification agreement. The indemnification agreements also require us, if so requested, to advance within 30 days of such request all reasonable fees, expenses, charges and other costs that such director or officer incurred, provided that such person will return any such advance if it is ultimately determined that such person is not entitled to indemnification by us. Any claims for indemnification by our directors and officers may reduce our available funds to satisfy successful third-party claims and may reduce the amount of money available to us.
If our internal controls over financial reporting are not considered effective, our business and stock price could be adversely affected.
Section 404 of the Sarbanes-Oxley Act of 2002 requires us to evaluate the effectiveness of our internal controls over financial reporting as of the end of each fiscal year and to include a management report assessing the effectiveness of our internal controls over financial reporting in our Form 10-K for that fiscal year. Section 404 also requires our independent registered public accounting firm to attest to, and report on, our internal controls over financial reporting. Our management, including our Chief Executive Officer and Chief Financial Officer, does not expect that our internal controls over financial
reporting will prevent all errors and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud involving a company have been, or will be, detected. The design of any system of controls is based in part on certain assumptions about the likelihood of future events, and we cannot assure you that any design will succeed in achieving its stated goals under all potential future conditions. Over time, controls may become ineffective because of changes in conditions or deterioration in the degree of compliance with policies or procedures. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected. We cannot assure you that we or our independent registered public accounting firm will not identify a material weakness in our internal controls in the future. A material weakness in our internal controls over financial reporting, such as described below, would require management and our independent registered public accounting firm to consider our internal controls as ineffective. If our internal controls over financial reporting are not considered effective, we may experience a loss of public confidence, which could have an adverse effect on our business and on the market price of our common stock.
Our management concluded that our internal controls over financial reporting were not effective as of December 31, 2019, and our auditors expressed an adverse opinion on the Company’s internal control over financial reporting as of December 31, 2019, due to a material weakness related to ineffective information technology general controls. We cannot provide assurances that a material weakness will be effectively remediated or that additional material weaknesses will not occur in the future. If we fail to maintain an effective system of internal controls, we may not be able to accurately report our financial results, prevent fraud, or maintain investor confidence.
Internal controls related to the operation of technology systems are critical to maintaining adequate internal control over financial reporting. As discussed in Part II, Item 9A of this report, management identified a material weakness in internal control related to ineffective information technology general controls (ITGCs) in the areas of user access, information security policies, and program change-management over certain information technology (IT) systems that support the Company’s financial reporting processes. As a result, management concluded that our internal control over financial reporting was not effective as of December 31, 2019. We are implementing remedial measures and, while there can be no assurance that our efforts will be successful, we plan to remediate the material weakness during fiscal year 2020 and we plan to monitor these changes throughout the year to ensure that new controls are operating effectively. These measures will result in additional technology and other expenses. If we are unable to remediate the material weakness, or are otherwise unable to maintain effective internal control over financial reporting or disclosure controls and procedures, our ability to record, process and report financial information accurately, and to prepare financial statements within required time periods, could be adversely affected, which could subject us to litigation or investigations requiring management resources and payment of legal and other expenses, which could negatively affect investor confidence in our financial statements and adversely impact our stock price.
ITEM 1B. UNRESOLVED STAFF COMMENTS
Not applicable.
ITEM 2. PROPERTIES
We lease the property for our corporate headquarters and all of the properties on which we own or manage clinics. As of December 31, 2019, we leased 65 facilities in which we operate or intend to operate clinics.
Our corporate headquarters are located at 16767 North Perimeter Drive, Suite 110, Scottsdale, Arizona 85260. The term of our lease for this location expires on December 31, 2025. The primary functions performed at our corporate headquarters are financial, accounting, treasury, marketing, operations, human resources, information systems support and legal.
We are also obligated under non-cancellable leases for the clinics which we own or manage. Our clinics are on average 1,200 square feet. Our clinic leases generally have an initial term of five years, include one to two options to renew for terms of five years, and require us to pay a proportionate share of real estate taxes, insurance, common area maintenance charges and other operating costs.
ITEM 3. LEGAL PROCEEDINGS
In the normal course of business, we are party to litigation from time to time. We maintain insurance to cover certain actions and believe that resolution of such litigation will not have a material adverse effect on the Company.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Beginning November 11, 2014, our common stock is traded on the NASDAQ Capital Market under the symbol “JYNT.”
Holders
As of December 31, 2019, there were approximately 10 holders of record of our common stock and 13,882,932 shares of our common stock outstanding.
Dividends
Since our initial public offering, we have not declared nor paid dividends on our common stock, and we do not expect to pay cash dividends on our common stock in the foreseeable future.
ITEM 6. SELECTED FINANCIAL DATA
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| Consolidated Statement of Operations Data: | | | (as adjusted) |
| (in thousands, except per share data) | | | |
| Total revenues | $ | 48,451 | | | $ | 36,662 | |
| Cost of revenues | 5,566 | | | 4,310 | |
| Selling, general and administrative expense | 39,356 | | | 31,614 | |
| Income from operations | 3,415 | | | 143 | |
| Net income | 3,324 | | | 147 | |
| Basic earnings per share | $ | 0.24 | | | $ | 0.01 | |
| Diluted earnings per share | $ | 0.23 | | | $ | 0.01 | |
| Weighted average shares outstanding used in computing | | | |
| Basic earnings per share | 13,819,149 | | | 13,669,107 | |
| Diluted earnings per share | 14,467,567 | | | 14,031,717 | |
| Non-GAAP Financial Data: | | | |
| Net income | 3,324 | | | 147 | |
| Net interest | 62 | | | 47 | |
| Depreciation and amortization expense | 1,899 | | | 1,556 | |
| Tax expense (benefit) | 49 | | | (38) | |
| EBITDA | 5,334 | | | 1,712 | |
| Stock compensation expense | 721 | | | 628 | |
| Acquisition related expenses | 47 | | | 4 | |
| Loss on disposition or impairment | 114 | | | 595 | |
| Bargain purchase gain | (19) | | | (13) | |
| Adjusted EBITDA | $ | 6,197 | | | $ | 2,926 | |
| | | | | | | | | | | |
| As of December 31, | | |
| 2019 | | 2018 |
| Consolidated Balance Sheet Data: | | | (as adjusted) |
| (in thousands) | | | |
| Cash and cash equivalents | $ | 8,456 | | | $ | 8,717 | |
| Property and equipment | 6,582 | | | 3,658 | |
| Deferred franchise costs | 4,393 | | | 3,489 | |
| Goodwill and intangible assets | 7,370 | | | 4,859 | |
| Operating lease right-of-use asset | 12,487 | | | — | |
| Other assets | 4,418 | | | 2,705 | |
| Total assets | 43,706 | | | 23,428 | |
| Deferred revenue | 18,304 | | | 16,139 | |
| Operating lease liability - current and non-current | 14,214 | | | — | |
| Other liabilities | 5,467 | | | 6,561 | |
| Total liabilities | 37,985 | | | 22,700 | |
| Stockholders' equity | $ | 5,721 | | | $ | 728 | |
(1)Adjusted EBITDA consists of net income before interest, income taxes, depreciation and amortization, acquisition related expenses, stock-based compensation expense, bargain purchase gain, and loss on disposition or impairment. We have provided Adjusted EBITDA because it is a non-GAAP measure of financial performance commonly used for comparing companies in our industry. You should not consider Adjusted EBITDA as a substitute for operating profit as an indicator of our operating performance or as an alternative to cash flows from operating activities as a measure of liquidity. We may calculate Adjusted EBITDA differently from other companies.
We believe that the use of Adjusted EBITDA provides an additional tool for investors to use in evaluating ongoing operating results and trends and in comparing our financial measures with other outpatient medical clinics, which may present similar non-GAAP financial measures to investors. In addition, you should be aware when evaluating Adjusted EBITDA that in the future we may incur expenses similar to those excluded when calculating these measures. Our presentation of these measures should not be construed as an inference that our future results will be unaffected by unusual or non-recurring items. Our computation of Adjusted EBITDA may not be comparable to other similarly titled measures computed by other companies, because all companies do not calculate Adjusted EBITDA in the same manner.
Our management does not consider Adjusted EBITDA in isolation or as an alternative to financial measures determined in accordance with GAAP. The principal limitation of Adjusted EBITDA is that it excludes significant expenses and income that are required by GAAP to be recorded in our financial statements. Some of these limitations are:
a.Adjusted EBITDA does not reflect our cash expenditures, or future requirements, for capital expenditures or contractual commitments;
b.Adjusted EBITDA does not reflect changes in, or cash requirements for, our working capital needs;
c.Adjusted EBITDA does not reflect the interest expense, or the cash requirements necessary to service interest or principal payments, on our debts;
d.Although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future, and Adjusted EBITDA does not reflect any cash requirements for such replacements;
e.Adjusted EBITDA does not reflect the bargain purchase gain, which represents the excess of the fair value of net assets acquired over the purchase consideration; and
f.Adjusted EBITDA does not reflect the loss on disposition or impairment, which represents the impairment of assets as of the reporting date. We do not consider this to be indicative of our ongoing operations
Because of these limitations, Adjusted EBITDA should not be considered in isolation or as a substitute for performance measures calculated in accordance with GAAP. We compensate for these limitations by relying primarily on our GAAP results
and using Adjusted EBITDA only supplementally. You should review the reconciliation of net income to Adjusted EBITDA above and not rely on any single financial measure to evaluate our business. The table above reconciles net income to Adjusted EBITDA for the years ended December 31, 2019 and 2018.
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion and analysis of the results of operations and financial condition of The Joint Corp. for the years ended December 31, 2019 and 2018 should be read in conjunction with the consolidated financial statements and the notes thereto, and other financial information contained elsewhere in this Form 10-K.
Overview
Our principal business is to develop, own, operate, support and manage chiropractic clinics through franchising and the sale of regional developer rights and through direct ownership and management arrangements throughout the United States.
We seek to be the leading provider of chiropractic care in the markets we serve and to become the most recognized brand in our industry through the rapid and focused expansion of chiropractic clinics in key markets throughout North America and potentially abroad.
Key Performance Measures. We receive monthly performance reports from our system and our clinics which include key performance indicators per clinic including gross sales, same-store Comp Sales, number of new patients, conversion percentage, and member attrition. In addition, we review monthly reporting related to clinic openings, clinic license sales, and various earnings metrics in the aggregate and per clinic. We believe these indicators provide us with useful data with which to measure our performance and to measure our franchisees’ and clinics’ performance.
Key Clinic Development Trends. As of December 31, 2019, we and our franchisees operated 513 clinics, of which 453 were operated by franchisees and 60 were operated as company-owned or managed clinics. Of the 60 company-owned or managed clinics, 20 were constructed and developed by us, and 40 were acquired from franchisees.
Our current strategy is to grow through the sale and development of additional franchises, build upon our regional developer strategy, and continue to expand our corporate clinic portfolio within clustered locations in a deliberate and measured manner. The number of franchise licenses sold for the year ended December 31, 2019 increased to 126 licenses, up from 99 and 37 licenses for the years ended December 31, 2018 and 2017, respectively. We ended 2019 with 21 regional developers who were responsible for 89% of the 126 licenses sold during the year. The growth reflects the power of the regional developer program to accelerate the number of clinics sold, and eventually opened, across the country.
In addition, we believe that we can accelerate the development of, and revenue generation from, company-owned or managed clinics through the further selective acquisition of existing franchised clinics and opening of greenfield units. We will seek to acquire existing franchised clinics that meet our criteria for demographics, site attractiveness, proximity to other clinics and additional suitability factors.
We believe that The Joint has a sound concept, benefiting from the fundamental changes taking place in the manner in which Americans access chiropractic care and their growing interest in seeking effective, affordable natural solutions for general wellness. These trends join with the strong preference we have seen among chiropractic doctors to reject the insurance-based model to produce a combination that benefits the consumer and the service provider alike. We believe that these forces create an important opportunity to accelerate the growth of our network.
Significant Events and/or Recent Developments
We continue to deliver on our strategic initiatives and to progress toward sustained profitability.
For the year ended December 31, 2019:
•Comp Sales of clinics that have been open for at least 13 full months increased 25%.
•Comp Sales for mature clinics open 48 months or more increased 19%.
•System-wide sales for all clinics open for any amount of time grew 33%.
We saw over 585,000 new patients in 2019, an increase of 26% from our new patient count in 2018, with approximately 26% of those new patients having never been to a chiropractor before. We are not only increasing our percentage of market share, but expanding the chiropractic market. These factors, along with continued leverage of our operating expenses, drove improvement in our bottom line.
On February 4, 2019, we entered into an agreement under which we repurchased the right to develop franchises in various counties in South Carolina and Georgia. The total consideration for the transaction was $681,500. We carried a deferred revenue balance associated with these transactions of $44,334, representing license fees collected upon the execution of the regional developer agreements. We accounted for the termination of development rights associated with unsold or undeveloped franchises as a cancellation, and the associated deferred revenue was netted against the aggregate purchase price.
On March 4, 2019, we entered into a regional developer agreement for a number of counties in the states of Virginia, Pennsylvania and West Virginia for $290,000. The development schedule requires a minimum of 40 clinics open over a ten-year period.
For the year ended December 31, 2019, we acquired eight clinics for approximately $3.1 million and constructed and developed five new corporate clinics.
Factors Affecting Our Performance
Our operating results may fluctuate significantly as a result of a variety of factors, including the timing of new clinic sales, openings, closures, markets in which they are contained and related expenses, general economic conditions, consumer confidence in the economy, consumer preferences, and competitive factors.
Significant Accounting Polices and Estimates
The preparation of consolidated financial statements requires us to make estimates and assumptions. These estimates and assumptions affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements, and the reported amounts of revenues and expenses during the reporting period. We base our accounting estimates on historical experience and other factors that we believe to be reasonable under the circumstances. Actual results could differ from those estimates. We have discussed the development and selection of significant accounting policies and estimates with our Audit Committee. In addition, we have restated prior period financial statements as discussed below.
Intangible Assets
Intangible assets consist primarily of re-acquired franchise and regional developer rights and customer relationships. We amortize the fair value of re-acquired franchise rights over the remaining contractual terms of the re-acquired franchise rights at the time of the acquisition, which range from three years to eight years. In the case of regional developer rights, we amortize the acquired regional developer rights over the remaining contractual terms at the time of the acquisition, which range from three to seven years. The fair value of customer relationships is amortized over their estimated useful life of two years.
Goodwill
Goodwill consists of the excess of the purchase price over the fair value of tangible and identifiable intangible assets acquired in the acquisitions of franchises. Goodwill and intangible assets deemed to have indefinite lives are not amortized but are subject to annual impairment tests. As required, we perform an annual impairment test of goodwill as of the first day of the fourth quarter or more frequently if events or circumstances change that would more likely than not reduce the fair value of a reporting unit below its carrying value. No impairments of goodwill were recorded for the years ended December 31, 2019 and 2018.
Long-Lived Assets
We review our long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying amount of the asset may not be recovered. We look primarily to estimated undiscounted future cash flows in its assessment of whether or not long-lived assets are recoverable. No impairments of long-lived assets were recorded for the year ended December 31, 2019. We recorded an impairment of approximately $343,000 in long-lived assets for the year ended December 31, 2018.
Stock-Based Compensation
The Company accounts for share-based payments by recognizing compensation expense based upon the estimated fair value of the awards on the date of grant. The Company determines the estimated grant-date fair value of restricted shares using the closing price on the date of the grant and the grant-date fair value of stock options using the Black-Scholes-Merton model. In order to calculate the fair value of the options, certain assumptions are made regarding the components of the model, including risk-free interest rate, volatility, expected dividend yield and expected option life. Changes to the assumptions could cause significant adjustments to the valuation. The Company recognizes compensation costs ratably over the period of service using the straight-line method.
Revenue Recognition
We generate revenue primarily through our company-owned and managed clinics, royalties, franchise fees, advertising fund, and through IT related income and computer software fees.
Revenues from Company-Owned or Managed Clinics. We earn revenue from clinics that we own and operate or manage throughout the United States. In those states where we own and operate the clinic, revenues are recognized when services are performed. We offer a variety of membership and wellness packages which feature discounted pricing as compared with our single-visit pricing. Amounts collected in advance for membership and wellness packages are recorded as deferred revenue and recognized when the service is performed. We recognize a contract liability (or a deferred revenue liability) related to the prepaid treatment plans for which we have an ongoing performance obligation. We recognize this contract liability, and recognize revenue, as the patient consumes his or her visits related to the package and we perform the services. Based on a historical lag analysis and an evaluation of legal obligation by jurisdiction, we concluded that any remaining contract liability that exists after 12 to 24 months from transaction date will be deemed breakage. Breakage revenue is recognized only at that point, when the likelihood of the patient exercising his or her remaining rights becomes remote.
Royalties and Advertising Fund Revenue. We collect royalties, as stipulated in the franchise agreement, equal to 7% of gross sales and a marketing and advertising fee currently equal to 2% of gross sales. Royalties, including franchisee contributions to advertising funds, are calculated as a percentage of clinic sales over the term of the franchise agreement. The franchise agreement royalties, inclusive of advertising fund contributions, represent sales-based royalties that are related entirely to our performance obligation under the franchise agreement and are recognized as franchisee clinic level sales occur. Royalties are collected bi-monthly two working days after each sales period has ended.
Franchise Fees. We require the entire non-refundable initial franchise fee to be paid upon execution of a franchise agreement, which typically has an initial term of ten years. Initial franchise fees are recognized ratably on a straight-line basis over the term of the franchise agreement. Our services under the franchise agreement include: training of franchisees and staff, site selection, construction/vendor management and ongoing operations support. We provide no financing to franchisees and offer no guarantees on their behalf. The services we provide are highly interrelated with the franchise license and as such are considered to represent a single performance obligation.
Software Fees. We collect a monthly fee for use of our proprietary or selected chiropractic or customer relationship management software, computer support, and internet services support. These fees are recognized ratably on a straight-line basis over the term of the respective franchise agreement.
Regional Developer Fees. During 2011, we established a regional developer program to engage independent contractors to assist in developing specified geographical regions. Under the original program, regional developers paid a license fee for each franchise they received the right to develop within the region. In 2017, the program was revised to grant exclusive geographical territory and establish a minimum development obligation within that defined territory. Regional developer fees are non-refundable and are recognized as revenue ratably on a straight-line basis over the term of the regional developer agreement, which is considered to begin upon the execution of the agreement. Our services under regional developer agreements include site selection, grand opening support for the clinics, sales support for identification of qualified franchisees, general operational support and marketing support to advertise for ownership opportunities. The services we provide are highly interrelated with the development of the territory and the resulting franchise licenses sold by the regional developer and as such are considered to represent a single performance obligation. In addition, regional developers receive fees which are funded by the initial franchise fees collected from franchisees upon the sale of franchises within their exclusive geographical territory and a royalty of 3% of sales generated by franchised clinics in their exclusive geographical territory. Fees related to the sale of franchises within their exclusive geographical territory are initially deferred as deferred franchise costs and are recognized as an expense in franchise cost of revenues when the respective revenue is recognized, which is generally over the term of the related franchise agreement.
Royalties of 3% of sales generated by franchised clinics in their regions are also recognized as franchise cost of revenues as franchisee clinic level sales occur.
Leases
We adopted, effective the first quarter of 2019, accounting guidance related to leases. The new guidance, among other changes, requires lessees to recognize a right-of-use ("ROU") asset and a lease liability in the balance sheet for most leases, but retains an expense recognition model similar to the previous guidance. The lease liability is measured at the present value of the fixed lease payments over the lease term and the ROU asset is measured at the lease liability amount, adjusted for lease prepayments, lease incentives received and the lessee’s initial direct costs. Determining the lease term and amount of lease payments to include in the calculation of the ROU asset and lease liability for leases containing options requires the use of judgment to determine whether the exercise of an option is reasonably certain and if the optional period and payments should be included in the calculation of the associated ROU asset and liability. In making this determination, all relevant economic factors are considered that would compel us to exercise or not exercise an option. When available, we use the rate implicit in the lease to discount lease payments; however, the rate implicit in the lease is not readily determinable for substantially all of our leases. In such cases, we estimate our incremental borrowing rate as the interest rate we would pay to borrow an amount equal to the lease payments over a similar term, with similar collateral as in the lease, and in a similar economic environment. We estimate these rates using available evidence such as rates imposed by third-party lenders in recent financings or observable risk-free interest rate and credit spreads for commercial debt of a similar duration, with credit spreads correlating to our estimated creditworthiness.
For operating leases that include rent holidays and rent escalation clauses, we recognize lease expense on a straight-line basis over the lease term from the date we take possession of the leased property. Pre-opening costs are recorded as incurred in general and administrative expenses. We record the straight-line lease expense and any contingent rent, if applicable, in general and administrative expenses on the consolidated statements of operations. Many of our leases also require us to pay real estate taxes, common area maintenance costs and other occupancy costs which are also included in general and administrative expenses on the consolidated statements of operations.
Results of Operations
The following discussion and analysis of our financial results encompasses our consolidated results and results of our two business segments: Corporate Clinics and Franchise Operations.
Prior Period Financial Statement Correction of Immaterial Error
Certain states in which we manage clinics regulate the practice of chiropractic care and require that chiropractic services be provided by legal entities organized under state laws as professional corporations or PCs. The PCs are variable interest entities (“VIEs”) as defined by Accounting Standards Codification 810, Consolidations (“ASC 810”). During the first quarter of 2019, we reassessed the governance structure and operating procedures of the PCs and determined that we have the power to control certain significant non-clinical activities of the PCs, as defined by ASC 810. Therefore, we are the primary beneficiary of the VIEs, and per ASC 810, must consolidate the VIEs. Prior to 2019, we did not consolidate the PCs. We concluded the previous accounting policy to not consolidate the PCs was an immaterial error and determined that the PCs should be consolidated. The adjustments resulted in an increase to revenues from company clinics and a corresponding increase to general and administrative expenses. The adjustments had no impact on net income, except when the PC had sold treatment packages and wellness plans. Revenue from these treatment packages and wellness plans are now deferred and will be recognized when patients use their visits. Please see Note 1, “Nature of Operations and Summary of Significant Accounting Policies,” in the Notes to Consolidated Financial Statements included in Item 8 of this report for further discussion. We corrected these immaterial errors by restating the 2018 consolidated financial statements as presented below.
Total Revenues
Components of revenues for the year ended December 31, 2019, as compared to the year ended December 31, 2018, are as follows:
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| Revenues: | | | (as adjusted) | | | | |
| Revenues from company-owned or managed clinics | $ | 25,807,584 | | | $ | 19,545,276 | | | $ | 6,262,308 | | | 32.0 | % |
| Royalty fees | 13,557,170 | | | 10,141,036 | | | 3,416,134 | | | 33.7 | % |
| Franchise fees | 1,791,545 | | | 1,688,039 | | | 103,506 | | | 6.1 | % |
| Advertising fund revenue | 3,884,055 | | | 2,862,244 | | | 1,021,811 | | | 35.7 | % |
| Software fees | 1,865,779 | | | 1,290,135 | | | 575,644 | | | 44.6 | % |
| Regional developer fees | 803,849 | | | 599,370 | | | 204,479 | | | 34.1 | % |
| Other revenues | 740,918 | | | 535,560 | | | 205,358 | | | 38.3 | % |
| Total revenues | $ | 48,450,900 | | | $ | 36,661,660 | | | $ | 11,789,240 | | | 32.2 | % |
The reasons for the significant changes in our components of total revenues are as follows:
Consolidated Results
•Total revenues increased by $11.8 million, primarily due to the continued revenue growth of our company-owned or managed clinics portfolio and continued expansion and revenue growth of our franchise base.
Corporate Clinics
•Revenues from company-owned or managed clinics increased, primarily due to improved same-store sales growth, as well as due to the expansion of our corporate-owned or managed clinics portfolio.
Franchise Operations
•Royalty fees and advertising fund revenue increased, due to an increase in the number of franchised clinics in operation along with continued sales growth in existing franchised clinics. As of December 31, 2019, and 2018, there were 453 and 394 franchised clinics in operation, respectively.
•Franchise fees increased due to an increase in executed franchise agreements, as these fees are recognized ratably over the term of the respective franchise agreement. For the year ended December 31, 2019, there were 126 executed franchise license sales or letters-of-intent, compared to 99 for the year ended December 31, 2018.
•Regional developer fees increased due to the sale of additional developer territories and the related revenue recognition over the life of the regional developer agreements. We sold three new regional developer territories in 2019 and four new territories in 2018. Given the ratable recognition of the revenue, the agreements executed during the course of 2018 now have a full year of recognition in 2019.
•Software fees revenue increased due to an increase in our franchise clinic base and the related revenue recognition over the term of the franchise agreement as described above.
•Other revenues primarily consist of merchant income associated with credit card transactions.
Cost of Revenues
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| Cost of Revenues | 5,565,917 | | | 4,310,249 | | | $ | 1,255,668 | | | 29.1 | % |
For the year ended December 31, 2019, as compared with the year ended December 31, 2018, the total cost of revenues increased primarily due to an increase in regional developer royalties of $1.0 million, which is in line with an increase in
franchise royalty revenues of 34% coupled with a larger portion of our franchise base operating in regional developer territories.
Selling and Marketing Expenses
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| Selling and Marketing Expenses | 6,913,709 | | | 4,819,555 | | | $ | 2,094,154 | | | 43.5 | % |
Selling and marketing expenses increased $2.1 million for the year ended December 31, 2019, as compared to the year ended December 31, 2018, driven by an increase in advertising fund expenditures from a larger franchise base and increased local marketing expenditures by the company-owned or managed clinics.
Depreciation and Amortization Expenses
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| Depreciation and Amortization Expenses | 1,899,257 | | | 1,556,240 | | | $ | 343,017 | | | 22.0 | % |
Depreciation and amortization expenses increased for the year ended December 31, 2019, as compared to the year ended December 31, 2018, primarily due to the amortization of intangibles related to the 2019 acquisitions.
General and Administrative Expenses
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| | | (as adjusted) | | | | | |
| General and Administrative Expenses | 30,543,030 | | | 25,238,121 | | | $ | 5,304,909 | | | 21.0 | % |
General and administrative expenses increased during the year ended December 31, 2019, compared to the year ended December 31, 2018, primarily due to an increase in payroll and related expenses, as well as operating expenses to support continued clinic count and revenue growth in both operating segments. As a percentage of revenue, general and administrative expenses during the year ended December 31, 2019 and 2018 were 63% and 69%, respectively, reflecting improved leverage of our operating model.
Income from Operations
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from | | Percent Change |
| 2019 | | 2018 | | Prior Year | | from Prior Year |
| | | (as adjusted) | | | | | |
| Income from Operations | 3,414,635 | | | 142,561 | | | $ | 3,272,074 | | | 2,295.2 | % |
Consolidated Results
Consolidated income from operations increased by $3.3 million for the year ended December 31, 2019 compared to the year ended December 31, 2018, primarily driven by a $2.9 million improvement in operating income in the franchise operations segment and an increase in operating income from the corporate clinic segment of $1.9 million, partially offset by an increase in unallocated corporate segment of $1.5 million discussed below.
Corporate Clinics
Our corporate clinics segment had income from operations of $3.4 million for the year ended December 31, 2019, an increase of $1.9 million compared to income from operations of $1.5 million for the year ended December 31, 2018. This increase was primarily due to:
•An increase in revenues of $6.3 million from company-owned or managed clinics; partially offset by
•A $4.4 million increase in operating expenses, primarily in general and administrative expenses. The increase in general and administrative expenses is primarily driven by an increase in payroll-related expenses due to a higher head count to support the expansion of our corporate clinic portfolio.
Franchise Operations
Our franchise operations segment had income from operations of $11.0 million for the year ended December 31, 2019, an increase of $2.9 million, compared to income from operations of $8.1 million for the year ended December 31, 2018. This increase was primarily due to:
•An increase of $5.5 million in total revenues; partially offset by
•An increase of $1.2 million in cost of revenues primarily due to an increase in regional developer royalties and an increase of $1.4 million in operating expenses, primarily due to an increase in selling and marketing expenses resulting from a larger franchise base.
Income Tax Expense (Benefit)
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | Change from Prior Year | | Percent Change from Prior Year |
| 2019 | | 2018 | | | | |
| Income Tax Expense (Benefit) | 48,706 | | | (37,728) | | | $ | 86,434 | | | (229.1) | % |
For the years ended December 31, 2019 and 2018, the effective tax rates were 1.4% and (34.6)%, respectively. The increase in our effective tax rate is primarily due to changes in pre-tax income and the decrease to the valuation allowance during the year ended December 31, 2019, as compared to year ended December 31, 2018. Please see Note 11, “Income Taxes” in the Notes to Consolidated Financial Statements included in Item 8 of this report for further discussion.
Liquidity and Capital Resources
Sources of Liquidity
From 2012 until November 2014, when we completed an initial public offering (“IPO”), we financed our business primarily through existing cash on hand and cash flows from operations.
On November 14, 2014, we completed our IPO of 3,000,000 shares of common stock at a price to the public of $6.50 per share. As a result of the IPO, we received aggregate net proceeds, after deducting underwriting discounts, commissions and other offering expenses, of approximately $17.1 million. On November 18, 2014, our underwriters exercised their option to purchase 450,000 additional shares of common stock to cover over-allotments, pursuant to which we received aggregate net proceeds of approximately $2.7 million.
On November 25, 2015, we completed our follow-on public offering of 2,272,727 shares of our common stock at a price to the public of $5.50 per share. On December 30, 2015, our underwriters exercised their over-allotment option to purchase an additional 340,909 shares of common stock to cover over-allotments pursuant to which we received aggregate net proceeds of approximately $13.0 million.
We have used a significant amount of the net proceeds from our public offerings for the development of company-owned or managed clinics. We accomplished this by developing new clinics and by repurchasing existing franchises. In addition, we have used proceeds from our offerings to repurchase existing regional developer licenses and to continue to expand our franchised clinic business. We are holding the remaining net proceeds in cash or short-term bank deposits.
As of December 31, 2019, we had cash and short-term bank deposits of $8.5 million. We generated $7.5 million of cash flow from operating activities in the year ended December 31, 2019. We will continue to preserve cash, and while we have resumed the acquisition and development of company-owned or managed clinics, we have progressed, and plan to continue to progress, at a measured pace, targeting geographic clusters where we are able to increase efficiencies through a consolidated real estate penetration strategy, leverage cooperative advertising and marketing and attain general corporate and administrative operating efficiencies.
In January 2017, we executed a credit and security agreement which provided a credit facility of up to $5.0 million, of which we drew $1.0 million during 2017. This balance remained outstanding during 2018 and most of 2019, which was repaid in full on December 20, 2019.
In February 2020, we executed a line of credit agreement which provides a credit facility of up to $7.5 million, including a $2.0 million revolver and $5.5 million development line of credit. Please see Note 14, “Subsequent Events” in the Notes to Consolidated Financial Statements included in Item 8 of this report for further discussion.
In addition to $8.5 million of unrestricted cash on hand as of December 31, 2019 and the available borrowings on the new line of credit, our principal sources of liquidity are expected to be cash flows from operations, proceeds from debt financings or equity issuances, and/or proceeds from the sale of assets. We expect our available cash and cash flows from operations, debt financings or equity issuances, or proceeds from the sale of assets to be sufficient to fund our short-term working capital requirements. Our long-term capital requirements, primarily for acquisitions and other corporate initiatives, could be dependent on our ability to access additional funds through the debt and/or equity markets. From time to time, we consider and evaluate transactions related to our portfolio and capital structure including debt financings, equity issuances, purchases and sales of assets, and other transactions. There can be no assurance that we will continue to generate cash flows at or above current levels or that we will be able to obtain the capital necessary to meet our short and long-term capital requirements.
Analysis of Cash Flows
Net cash provided by operating activities was $7.5 million for the year ended December 31, 2019, compared to net cash provided by operating activities of $5.5 million for the year ended December 31, 2018. The change was attributable primarily to improved operating income over the prior year.
Net cash used in investing activities was $7.1 million and $1.2 million during the years ended December 31, 2019 and 2018, respectively. For the year ended December 31, 2019, this included acquisition of business of $3.1 million, purchases of property and equipment of $3.5 million, and reacquisition and termination of regional developer rights of $0.7 million, partially offset by payments received on notes receivable of $0.1 million. For the year ended December 31, 2018, this included acquisition of business of $0.1 million, purchases of property and equipment of $1.1 million, and reacquisition and termination of regional developer rights of $0.3 million, partially offset by payments received on notes receivable of $0.2 million.
Net cash (used in) provided by financing activities was ($0.6) million and $0.3 million during the years ended December 31, 2019 and 2018, respectively. For the year ended December 31, 2019, this included proceeds from exercise of stock options of $0.5 million, which was more than offset by purchases of treasury stock under employee stock plans of approximately $21,000, payments of finance lease obligation of approximately $22,000, and repayments on notes payable of $1.1 million. For the year ended December 31, 2018, this included proceeds from exercise of stock options of $0.3 million partially offset by purchases of treasury stock under employee stock plans of approximately $5,000.
Recent Accounting Pronouncements
Please see Note 1, “Nature of Operations and Summary of Significant Accounting Policies” in the Notes to Consolidated Financial Statements included in Item 8 of this report for information regarding recently issued accounting pronouncements that may impact our financial statements.
Contractual Obligations and Risk
The following table summarizes our contractual obligations at December 31, 2019 and the effect that such obligations are expected to have on our liquidity and cash flows in future periods:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Payments Due by Fiscal Year | | | | | | | | | | | | |
| Total | | 2020 | | 2021 | | 2022 | | 2023 | | 2024 | | Thereafter |
| Operating leases | $ | 17,794,374 | | | 3,376,830 | | | 3,545,186 | | | 3,430,110 | | | 2,716,465 | | | 2,096,333 | | | 2,629,450 | |
| | | | | | | | | | | | | |
Off-Balance Sheet Arrangements
During the year ended December 31, 2019, we did not have any relationships with unconsolidated organizations or financial partnerships, such as structured finance or special purpose entities that were established for the purpose of facilitating off-balance sheet arrangements.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Not required for smaller reporting companies.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Report of Independent Registered Public Accounting Firm
To the Stockholders and Board of Directors of The Joint Corp. and Subsidiary and Affiliates
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheets of The Joint Corp. and subsidiary and affiliates (the “Company”) as of December 31, 2019 and 2018, and the related consolidated statements of operations and comprehensive income, stockholders’ equity, and cash flows for each of the years in the two year period ended December 31, 2019, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2019 and 2018, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2019, in conformity with accounting principles generally accepted in the United States of America.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (“PCAOB”), the Company’s internal control over financial reporting as of December 31, 2019, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”) and our report dated March 6, 2020 expressed an adverse opinion thereon.
Adoption of New Accounting Standards
As discussed in Note 1 to the consolidated financial statements, the Company has changed its method for accounting for leases in 2019 due to the adoption of the new lease standard. The Company adopted the new lease standard using a modified retrospective approach.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s consolidated financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Plante & Moran, PLLC
We have served as the Company’s auditor since 2013.
Denver, Colorado
March 6, 2020
Report of Independent Registered Public Accounting Firm
To the Stockholders and Board of Directors of The Joint Corp. and Subsidiary and Affiliates
Opinion on Internal Control Over Financial Reporting
We have audited The Joint Corp and subsidiary and affiliates (the “Company”) internal control over financial reporting as of December 31, 2019, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (the “COSO criteria”). In our opinion, because of the material weakness described below on the achievement of objectives of the control criteria, the Company has not maintained effective internal control over financial reporting as of December 31, 2019, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (“PCAOB”), the consolidated balance sheets of the Company and subsidiary and affiliates as of December 31, 2019 and 2018, and the related consolidated statements of operations and comprehensive income, stockholders’ equity, and cash flows for each of the two years in the period ended December 31, 2019, and the related notes (collectively referred to as “the consolidated the financial statements”) and our report dated March 6, 2020, expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Item 9A, Management’s Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit of internal control over financial reporting in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A material weakness is a deficiency, or a combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of the Company’s annual or interim financial statements will not be prevented or detected on a timely basis. The following material weakness has been identified and included in management’s assessment:
There were ineffective information technology general controls (ITGCs) in the areas of logical access, user administration, program change and information security policies over certain information technology (IT) systems that support the Company’s financial reporting processes. As a result, certain business process automated and manual controls that were dependent on the affected ITGCs were ineffective because they could have been adversely impacted.
This material weakness was considered in determining the nature, timing, and extent of audit tests applied in our audit of the 2019 financial statements, and this report does not affect our report dated March 6, 2020, on those financial statements.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ Plante & Moran, PLLC
Denver, Colorado
March 6, 2020
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED BALANCE SHEETS
| | | | | | | | | | | |
| December 31,
2019 | | December 31,
2018 |
| ASSETS | | | (as adjusted) |
| Current assets: | | | |
| Cash and cash equivalents | $ | 8,455,989 | | | $ | 8,716,874 | |
| Restricted cash | 185,888 | | | 138,078 | |
| Accounts receivable, net | 2,645,085 | | | 806,350 | |
| Income taxes receivable | — | | | 268 | |
| Notes receivable, net - current portion | 128,724 | | | 149,349 | |
| Deferred franchise costs - current portion | 765,508 | | | 611,047 | |
| Prepaid expenses and other current assets | 1,122,478 | | | 882,022 | |
| Total current assets | 13,303,672 | | | 11,303,988 | |
| Property and equipment, net | 6,581,588 | | | 3,658,007 | |
| Operating lease right-of-use asset | 12,486,672 | | | — | |
| Notes receivable net - net of current portion | — | | | 128,723 | |
| Deferred franchise costs, net of current portion | 3,627,225 | | | 2,878,163 | |
| Intangible assets, net | 3,219,791 | | | 1,634,060 | |
| Goodwill | 4,150,461 | | | 3,225,145 | |
| Deposits and other assets | 336,258 | | | 599,627 | |
| Total assets | $ | 43,705,667 | | | $ | 23,427,713 | |
| | | |
| LIABILITIES AND STOCKHOLDERS' EQUITY | | | |
| Current liabilities: | | | |
| Accounts payable | $ | 1,525,838 | | | $ | 1,253,274 | |
| Accrued expenses | 216,814 | | | 266,322 | |
| Co-op funds liability | 185,889 | | | 104,057 | |
| Payroll liabilities | 2,844,107 | | | 2,035,658 | |
| Notes payable - current portion | — | | | 1,100,000 | |
| Deferred rent - current portion | — | | | 136,550 | |
| Operating lease liability - current portion | 2,313,109 | | | | — | |
| Finance lease liability - current portion | 24,253 | | | | — | |
| Deferred franchise and regional developer fee revenue - current portion | 2,740,954 | | | 2,370,241 | |
| Deferred revenue from company clinics | 3,196,664 | | | 2,529,497 | |
| Other current liabilities | 518,686 | | | 477,528 | |
| Total current liabilities | 13,566,314 | | | 10,273,127 | |
| Deferred rent, net of current portion | — | | | 721,730 | |
| Operating lease liability - net of current portion | 11,901,040 | | | | — | |
| Finance lease liability - net of current portion | 34,398 | | | | — | |
| Deferred franchise and regional developer fee revenue, net of current portion | 12,366,322 | | | 11,239,221 | |
| Deferred tax liability | 89,863 | | | 76,672 | |
| Other liabilities | 27,230 | | | 389,362 | |
| Total liabilities | 37,985,167 | | | 22,700,112 | |
| Commitments and contingencies | | | |
| Stockholders' equity: | | | |
| Series A preferred stock, $0.001 par value; 50,000 shares authorized, 0 issued and outstanding, as of December 31, 2019 and 2018 | — | | | — | |
| Common stock, $0.001 par value; 20,000,000 shares authorized, 13,898,694 shares issued and 13,882,932 shares outstanding as of December 31, 2019 and 13,757,200 shares issued and 13,742,530 outstanding as of December 31, 2018 | 13,899 | | | 13,757 | |
| Additional paid-in capital | 39,454,937 | | | 38,189,251 | |
| Treasury stock 15,762 shares as of December 31, 2019 and 14,670 shares as of December 31, 2018, at cost | (111,041) | | | (90,856) | |
| Accumulated deficit | (33,637,395) | | | (37,384,651) | |
| | | | | | | | | | | |
| Total The Joint Corp. stockholders' equity | 5,720,400 | | | 727,501 | |
| Non-controlling Interest | 100 | | | 100 | |
| Total equity | 5,720,500 | | | 727,601 | |
| Total liabilities and stockholders' equity | $ | 43,705,667 | | | $ | 23,427,713 | |
Note: The Consolidated Balance Sheet as of December 31, 2018 has been derived from the audited consolidated financial statements, restated to reflect the consolidation of variable interest entities. In addition, during the quarter ended December 31, 2019, the Company recorded a correction of an immaterial error related to the adoption of ASC 606. The error was not material to the Company's Consolidated Financial Statements for any quarterly or annual period. See Note 1 of “Notes to Consolidated Financial Statements” under the heading “Prior Period Financial Statement Correction of Immaterial Error” for more details. The accompanying notes are an integral pat of these consolidated financial statements.
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED STATEMENTS OF OPERATIONS
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| | | (as adjusted) |
| Revenues: | | | |
| Revenues from company-owned or managed clinics | $ | 25,807,584 | | | $ | 19,545,276 | |
| Royalty fees | 13,557,170 | | | 10,141,036 | |
| Franchise fees | 1,791,545 | | | 1,688,039 | |
| Advertising fund revenue | 3,884,055 | | | 2,862,244 | |
| Software fees | 1,865,779 | | | 1,290,135 | |
| Regional developer fees | 803,849 | | | 599,370 | |
| Other revenues | 740,918 | | | 535,560 | |
| Total revenues | 48,450,900 | | | 36,661,660 | |
| Cost of revenues: | | | |
| Franchise cost of revenues | 5,159,778 | | | 3,956,530 | |
| IT cost of revenues | 406,139 | | | 353,719 | |
| Total cost of revenues | 5,565,917 | | | 4,310,249 | |
| Selling and marketing expenses | 6,913,709 | | | 4,819,555 | |
| Depreciation and amortization | 1,899,257 | | | 1,556,240 | |
| General and administrative expenses | 30,543,030 | | | 25,238,121 | |
| Total selling, general and administrative expenses | 39,355,996 | | | 31,613,916 | |
| Net loss on disposition or impairment | 114,352 | | | 594,934 | |
| Income from operations | 3,414,635 | | | 142,561 | |
| | | |
| Other income (expense): | | | |
| Bargain purchase gain | 19,298 | | | 13,198 | |
| Other (expense), net | (61,515) | | | (46,791) | |
| Total other (expense) | (42,217) | | | (33,593) | |
| | | |
| Income before income tax expense (benefit) | 3,372,418 | | | 108,968 | |
| | | |
| Income tax expense (benefit) | 48,706 | | | (37,728) | |
| | | |
| Net income and comprehensive income | $ | 3,323,712 | | | $ | 146,696 | |
| | | |
| Less: income attributable to the non-controlling interest | $ | — | | | $ | — | |
| | | |
| Net income attributable to The Joint Corp. stockholders | $ | 3,323,712 | | | $ | 146,696 | |
| | | |
| Earnings per share: | | | |
| Basic earnings per share | $ | 0.24 | | | $ | 0.01 | |
| Diluted earnings per share | $ | 0.23 | | | $ | 0.01 | |
| | | |
| Basic weighted average shares | 13,819,149 | | | 13,669,107 | |
| Diluted weighted average shares | 14,467,567 | | | 14,031,717 | |
Note: The Consolidated Statement of Operations for the year ended December 31, 2018 has been restated to reflect the consolidation of variable interest entities. In addition, during the quarter ended December 31, 2019, the Company recorded a correction of an immaterial error related to the adoption of ASC 606. The error was not material to the Company's Consolidated Financial Statements for any quarterly or annual period. See Note 1 of “Notes to Consolidated Financial
Statements” under the heading “Prior Period Financial Statement Correction of Immaterial Error” for more details. The accompanying notes are an integral part of these consolidated financial statements.
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED STATEMENTS OF CHANGES IN STOCKHOLDERS’ EQUITY
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Common Stock | | | | Additional
Paid In Capital | | Treasury Stock | | | | Accumulated
Deficit | | | | | |
| Shares | | Amount | | | | Shares | | Amount | | | | Total The Joint Corp. stockholder's equity | | Non-controlling Interest | Total |
| Balances, December 31, 2017 | 13,600,338 | | | $ | 13,600 | | | $ | 37,229,869 | | | 14,084 | | | $ | (86,045) | | | $ | (37,531,347) | | | $ | (373,923) | | | $ | 100 | | $ | (373,823) | |
| Stock-based compensation expense | — | | | — | | | 628,430 | | | — | | | — | | | — | | | 628,430 | | | — | | 628,430 | |
| Issuance of vested restricted stock | 61,700 | | | 62 | | | (62) | | | — | | | — | | | — | | | — | | | — | | — | |
| Exercise of stock options | 95,162 | | | | 95 | | | | 331,014 | | | | — | | | | — | | | | — | | | | 331,109 | | | | — | | 331,109 | |
| Purchases of treasury stock under employee stock plans | — | | | — | | | — | | | 586 | | | (4,811) | | | — | | | (4,811) | | | — | | (4,811) | |
| Net income | — | | | — | | | — | | | — | | | — | | | 146,696 | | | 146,696 | | | — | | 146,696 | |
| Balances, December 31, 2018 (as adjusted) | 13,757,200 | | | $ | 13,757 | | | $ | 38,189,251 | | | 14,670 | | | $ | (90,856) | | | $ | (37,384,651) | | | $ | 727,501 | | | $ | 100 | | $ | 727,601 | |
| Correction of immaterial error related to ASC 606 adoption | — | | | | — | | | | — | | | | — | | | | — | | | | 423,544 | | | | 423,544 | | | | — | | 423,544 | |
| Stock-based compensation expense | — | | | — | | | 720,651 | | | — | | | — | | | — | | | 720,651 | | | — | | 720,651 | |
| Issuance of vested restricted stock | 38,289 | | | 38 | | | (38) | | | — | | | — | | | — | | | — | | | — | | — | |
| Exercise of stock options | 103,205 | | | 104 | | | 545,073 | | | — | | | — | | | — | | | 545,177 | | | — | | 545,177 | |
| Purchases of treasury stock under employee stock plans | — | | | — | | | — | | | 1,092 | | | (20,185) | | | — | | | (20,185) | | | — | | (20,185) | |
| Net income | — | | | — | | | — | | | — | | | — | | | 3,323,712 | | | 3,323,712 | | | — | | 3,323,712 | |
| Balances, December 31, 2019 | 13,898,694 | | | $ | 13,899 | | | $ | 39,454,937 | | | 15,762 | | | $ | (111,041) | | | $ | (33,637,395) | | | $ | 5,720,400 | | | $ | 100 | | $ | 5,720,500 | |
Note: The Consolidated Statement of Changes in Stockholders’ Equity has been restated to reflect the consolidation of variable interest entities. In addition, during the quarter ended December 31, 2019, the Company recorded a correction of an immaterial error related to the adoption of ASC 606. The error was not material to the Company's Consolidated Financial Statements for any quarterly or annual period. See Note 1 of “Notes to Consolidated Financial Statements” under the heading “Prior Period Financial Statement Correction of Immaterial Error” for more details. The accompanying notes are an integral part of these consolidated financial statements.
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED STATEMENTS OF CASH FLOWS
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| | | (as adjusted) |
| Cash flows from operating activities: | | | |
| Net income | $ | 3,323,712 | | | $ | 146,696 | |
| Adjustments to reconcile net income to net cash provided by (used in) operating activities: | | | |
| Depreciation and amortization | 1,899,257 | | | 1,556,240 | |
| Net loss on disposition or impairment | 114,352 | | | 594,934 | |
| Net franchise fees recognized upon termination of franchise agreements | (113,944) | | | (227,950) | |
| Bargain purchase gain | (19,298) | | | (13,198) | |
| Deferred income taxes | 1,781 | | | (77,020) | |
| Stock based compensation expense | 720,651 | | | 628,430 | |
| Changes in operating assets and liabilities: | | | |
| Accounts receivable | (1,838,735) | | | (78,716) | |
| Prepaid expenses and other current assets | (240,188) | | | (339,948) | |
| Deferred franchise costs | (882,672) | | | (802,990) | |
| Deposits and other assets | 268,369 | | | 38,983 | |
| Accounts payable | 75,893 | | | 63,567 | |
| Accrued expenses | (64,758) | | | 177,768 | |
| Payroll liabilities | 808,449 | | | 1,168,228 | |
| Deferred revenue | 853,184 | | | 2,647,123 | |
| Other liabilities | 2,615,896 | | | (29,879) | |
| Net cash provided by operating activities | 7,521,949 | | | 5,452,268 | |
| | | |
| Cash flows from investing activities: | | | |
| Acquisition of business | (3,122,332) | | | (100,000) | |
| Purchase of property and equipment | (3,483,578) | | | (1,111,117) | |
| Reacquisition and termination of regional developer rights | (681,500) | | | (278,250) | |
| Payments received on notes receivable | 149,348 | | | 245,713 | |
| Net cash used in investing activities | (7,138,062) | | | (1,243,654) | |
| | | |
| Cash flows from financing activities: | | | |
| Payments of finance lease obligation | (21,954) | | | — | |
| Purchases of treasury stock under employee stock plans | (20,185) | | | (4,811) | |
| Proceeds from exercise of stock options | 545,177 | | | 331,109 | |
| Repayments on notes payable | (1,100,000) | | | — | |
| Net cash (used in) provided by financing activities | (596,962) | | | 326,298 | |
| | | |
| (Decrease) increase in cash | (213,075) | | | 4,534,912 | |
| Cash and restricted cash, beginning of period | 8,854,952 | | | 4,320,040 | |
| Cash and restricted cash, end of period | $ | 8,641,877 | | | $ | 8,854,952 | |
During the years ended December 31, 2019 and 2018, cash paid for income taxes was $65,064 and $29,522, respectively. During the years ended December 31, 2019 and 2018, cash paid for interest was $96,978 and $100,000, respectively.
Supplemental disclosure of non-cash activity:
As of December 31, 2019, accounts payable and accrued expenses include property and equipment purchases of $196,671, and $15,250, respectively. As of December 31, 2018, accounts payable and accrued expenses include property and equipment purchases of $121,038, and $1,595, respectively.
In connection with the acquisitions during the year ended December 31, 2019, the Company acquired $173,521 of property and equipment and intangible assets of $1,999,469, in exchange for $3,127,332 (of which $5,000 was in accounts payable as of December 31, 2019) to the sellers. Additionally, at the time of these transactions, the Company carried net deferred revenue of $40,805, representing unrecognized net franchise fees collected upon the execution of the franchise agreement. The Company netted this amount against the purchase price of the acquisitions (Note 2).
In connection with the Company's reacquisition and termination of regional developer rights during the year ended December 31, 2019, the Company had deferred revenue of $44,334 representing unrecognized license fees collected upon the execution of the regional developer agreements. The Company netted these amounts against the aggregate purchase price of the acquisitions (Note 8).
Note: The Consolidated Statements of Cash Flows has been restated to reflect the consolidation of variable interest entities. See Note 1 of “Notes to Consolidated Financial Statements” under the heading “Prior Period Financial Statement Correction of Immaterial Error” for more details. The accompanying notes are an integral part of these consolidated financial statements.
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1: Nature of Operations and Summary of Significant Accounting Policies
Basis of Presentation
These financial statements represent the consolidated financial statements of The Joint Corp. (“The Joint”), its variable interest entities (“VIEs”), and its wholly owned subsidiary, The Joint Corporate Unit No. 1, LLC (collectively, the “Company”). The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the amount of assets, liabilities, revenue, costs, expenses and other (expenses) income that are reported in the consolidated financial statements and accompanying disclosures. These estimates are based on management’s best knowledge of current events, historical experience, actions that the Company may undertake in the future and on various other assumptions that are believed to be reasonable under the circumstances. As a result, actual results may be different from these estimates. For a discussion of significant estimates and judgments made in recognizing revenue and accounting for leases, see Note 3, "Revenue Disclosures" and Note 12, "Commitments and Contingencies", respectively.
Prior Period Financial Statement Correction of Immaterial Error
Certain states in which the Company manages clinics regulate the practice of chiropractic care and require that chiropractic services be provided by legal entities organized under state laws as professional corporations or PCs. The PCs are VIEs as defined by Accounting Standards Codification 810, Consolidations (“ASC 810”). During the first quarter of 2019, the Company reassessed the governance structure and operating procedures of the PCs and determined that the Company has the power to control certain significant non-clinical activities of the PCs, as defined by ASC 810. Therefore, the Company is the primary beneficiary of the VIEs, and per ASC 810, must consolidate the VIEs. Prior to 2019, the Company did not consolidate the PCs. The Company concluded the previous accounting policy to not consolidate the PCs was an immaterial error and determined that the PCs should be consolidated. The adjustments resulted in an increase to revenues from company clinics and a corresponding increase to general and administrative expenses. The adjustments had no impact on net income, except when the PCs had sold treatment packages and wellness plans. Revenue from these treatment packages and wellness plans are now deferred and will be recognized when patients use their visits. The Company corrected this immaterial error by restating the 2018 consolidated financial statements and related notes included herein.
The immaterial impacts of this error correction for the fiscal year ended December 31, 2018 were as follows:
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED STATEMENTS OF OPERATIONS
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, 2018 | | Adjustments Due To VIE Consolidation | | Year Ended December 31, 2018 |
| (as reported) | | | | (as adjusted) |
| Revenues: | | | | | |
| Revenues from company-owned or managed clinics | $ | 14,672,865 | | | $ | 4,872,411 | | | $ | 19,545,276 | |
| Total revenues | 31,789,249 | | | 4,872,411 | | | 36,661,660 | |
| General and administrative expenses | 20,304,131 | | | 4,933,990 | | | 25,238,121 | |
| Total selling, general and administrative expenses | 26,679,926 | | | 4,933,990 | | | 31,613,916 | |
| Income from operations | 204,139 | | | (61,578) | | | 142,561 | |
| | | | | |
| Other income (expense): | | | | | |
| Bargain purchase gain | 58,006 | | | (44,808) | | | $ | 13,198 | |
| Total other income (expense) | 11,215 | | | (44,808) | | | $ | (33,593) | |
| | | | | |
| Income before income tax (benefit) expense | 215,354 | | | (106,386) | | | $ | 108,968 | |
| | | | | |
| Net income and comprehensive income | $ | 253,082 | | | (106,386) | | | $ | 146,696 | |
| | | | | |
| Earnings per share: | | | | | |
| Basic earnings per share | $ | 0.02 | | | (0.01) | | | $ | 0.01 | |
| Diluted earnings per share | $ | 0.02 | | | (0.01) | | | | $ | 0.01 | |
| | | | | |
| Basic weighted average shares | 13,669,107 | | | — | | | $ | 13,669,107 | |
| Diluted weighted average shares | 14,031,717 | | | — | | | $ | 14,031,717 | |
THE JOINT CORP. AND SUBSIDIARY AND AFFILIATES
CONSOLIDATED BALANCE SHEETS
| | | | | | | | | | | | | | | | | |
| December 31, 2018 | | Adjustments Due To VIE Consolidation | | December 31, 2018 |
| ASSETS | (as reported) | | | | (as adjusted) |
| Current assets: | | | | | |
| Accounts receivable, net | 1,213,707 | | | (407,357) | | | 806,350 | |
| Total current assets | 11,711,345 | | | (407,357) | | | 11,303,988 | |
| Goodwill | 2,916,426 | | | 308,719 | | | 3,225,145 | |
| Total assets | $ | 23,526,352 | | | $ | (98,639) | | | $ | 23,427,713 | |
| | | | | |
| LIABILITIES AND STOCKHOLDERS' EQUITY | | | | | |
| Current liabilities: | | | | | |
| Deferred revenue from company clinics | 994,493 | | | 1,535,004 | | | 2,529,497 | |
| Total current liabilities | 8,738,123 | | | 1,535,004 | | | 10,273,127 | |
| Total liabilities | 21,165,108 | | | 1,535,004 | | | 22,700,112 | |
| Commitments and contingencies | | | | | |
| Equity: | | | | | |
| The Joint Corp. stockholders' equity: | | | | | |
| Accumulated deficit | (35,750,908) | | | (1,633,743) | | | (37,384,651) | |
| Total The Joint Corp. stockholders' equity | 2,361,244 | | | (1,633,743) | | | 727,501 | |
| Non-controlling Interest | — | | | 100 | | | 100 | |
| Total equity | 2,361,244 | | | (1,633,643) | | | 727,601 | |
| Total liabilities and equity | $ | 23,526,352 | | | $ | (98,639) | | | $ | 23,427,713 | |
Correction of Immaterial Error - Effect of change in accounting principle
During the quarter ended December 31, 2019, the Company determined that it had improperly calculated the effect of change in accounting principle related to the adoption of Accounting Standards Codification 606 - Revenue from Contracts with Customers ("ASC 606"), which the Company adopted on January 1, 2018. This resulted in an overstatement of deferred franchise revenue and an understatement of deferred franchise costs. As a result, the Company recorded a $150 thousand reduction to franchise fee revenue and $70 thousand increase to franchise cost of revenue with a corresponding adjustment to deferred franchise revenue and deferred franchise costs related to the prior year and current year correction of an immaterial error related to the adoption of ASC 606.The error was not material to the Company's consolidated financial statements for any quarterly or annual period.
Nature of Operations
The Joint Corp., a Delaware corporation, was formed on March 10, 2010 for the principal purpose of franchising, developing and managing chiropractic clinics, selling regional developer rights and supporting the operations of franchised chiropractic clinics at locations throughout the United States of America. The franchising of chiropractic clinics is regulated by the Federal Trade Commission and various state authorities.
The following table summarizes the number of clinics in operation under franchise agreements and as company-owned or managed for the years ended December 31, 2019 and 2018:
| | | | | | | | | | | |
| Year Ended December 31, | | |
| Franchised clinics: | 2019 | | 2018 |
| Clinics open at beginning of period | 394 | | | 352 | |
| Opened during the period | 71 | | | 47 | |
| Sold during the period | (8) | | | (1) | |
| Closed during the period | (4) | | | (4) | |
| Clinics in operation at the end of the period | 453 | | | 394 | |
| | | | | | | | | | | |
| Year Ended December 31, | | |
| Company-owned or managed clinics: | 2019 | | 2018 |
| Clinics open at beginning of period | 48 | | | 47 | |
| Opened during the period | 5 | | | — | |
| Acquired during the period | 8 | | | 1 | |
| Closed during the period | (1) | | | — | |
| Clinics in operation at the end of the period | 60 | | | 48 | |
| | | |
| Total clinics in operation at the end of the period | 513 | | | 442 | |
| | | |
| Clinic licenses sold but not yet developed | 170 | | | 136 | |
| Executed letters of intent for future clinic licenses | 34 | | | 19 | |
Principles of Consolidation
The accompanying consolidated financial statements include the accounts of The Joint Corp. and its wholly-owned subsidiary, The Joint Corporate Unit No. 1, LLC, which was dormant for all periods presented. The Company consolidates VIEs in which the Company is the primary beneficiary in accordance with ASC 810. Non-controlling interests represent third-party equity ownership interests in VIEs.
All significant inter-affiliate accounts and transactions between The Joint and its VIEs have been eliminated in consolidation. Certain balances were reclassified from regional developer fees to other revenues for the year ended December 31, 2018 to conform to the current year presentation.
Comprehensive Income
Net income and comprehensive income are the same for the years ended December 31, 2019 and 2018.
Variable Interest Entities
An entity deemed to hold the controlling interest in a voting interest entity or deemed to be the primary beneficiary of a VIE is required to consolidate the VIE in its financial statements. An entity is deemed to be the primary beneficiary of a VIE if it has both of the following characteristics: (a) the power to direct the activities of a VIE that most significantly impact the VIE's economic performance and (b) the obligation to absorb the majority of losses of the VIE or the right to receive the majority of benefits from the VIE.
Certain states in which the Company manages clinics regulate the practice of chiropractic care and require that chiropractic services be provided by legal entities organized under state laws as professional corporations or PCs. In these states, the Company has entered into management services agreements with PCs under which the Company provides, on an exclusive basis, all non-clinical services of the chiropractic practice. Such PCs are VIEs, as fees paid by the PCs to the Company as its management service provider are considered variable interests because they are liabilities on the PC’s books and the fees do not meet all the following criteria: 1) The fees are compensation for services provided and are commensurate with the level of effort required to provide those services; 2) The decision maker or service provider does not hold other interests in the VIE that individually, or in the aggregate, would absorb more than an insignificant amount of the VIE’s expected losses or receive more than an insignificant amount of the VIE’s expected residual returns; 3) The service arrangement includes only terms, conditions, or amounts that are customarily present in arrangements for similar services negotiated at arm’s length. During the
first quarter of 2019, the Company reassessed the governance structure and operating procedures of the PCs and determined that the Company has the power to control certain significant non-clinical activities of the PCs, as defined by ASC 810, Therefore, the Company is the primary beneficiary of the VIEs, and per ASC 810, must consolidate the VIEs. The carrying amount of VIE assets and liabilities are immaterial as of December 31, 2019.
Cash and Cash Equivalents
The Company considers all highly liquid instruments purchased with an original maturity of three months or less to be cash equivalents. The Company continually monitors its positions with, and credit quality of, the financial institutions with which it invests. As of the balance sheet date and periodically throughout the period, the Company has maintained balances in various operating accounts in excess of federally insured limits. The Company has invested substantially all its cash in short-term bank deposits. The Company had no cash equivalents as of December 31, 2019 and 2018.
Restricted Cash
Restricted cash relates to cash that franchisees and company-owned or managed clinics contribute to the Company’s National Marketing Fund and cash that franchisees provide to various voluntary regional Co-Op Marketing Funds. Cash contributed by franchisees to the National Marketing Fund is to be used in accordance with the Company’s Franchise Disclosure Document with a focus on regional and national marketing and advertising.
Accounts Receivable
Accounts receivable primarily represent amounts due from franchisees for royalty fees. The Company considers a reserve for doubtful accounts based on the creditworthiness of the entity. The provision for uncollectible amounts is continually reviewed and adjusted to maintain the allowance at a level considered adequate to cover future losses. The allowance is management’s best estimate of uncollectible amounts and is determined based on specific identification and historical performance that the Company tracks on an ongoing basis. Actual losses ultimately could differ materially in the near term from the amounts estimated in determining the allowance. As of December 31, 2019, and 2018, the Company had an allowance for doubtful accounts of $0.
Deferred Franchise Costs
Deferred franchise costs represent commissions that are direct and incremental to the Company and are paid in conjunction with the sale of a franchise license. These costs are recognized as an expense, in franchise cost of revenues when the respective revenue is recognized, which is generally over the term of the related franchise agreement.
Property and Equipment
Property and equipment are stated at cost or for property acquired as part of franchise acquisitions at fair value at the date of closing. Depreciation is computed using the straight-line method over estimated useful lives of three to seven years. Leasehold improvements are amortized using the straight-line method over the shorter of the lease term or the estimated useful life of the assets.
Maintenance and repairs are charged to expense as incurred; major renewals and improvements are capitalized. When items of property or equipment are sold or retired, the related cost and accumulated depreciation are removed from the accounts and any gain or loss is included in income.
Capitalized Software
The Company capitalizes certain software development costs. These capitalized costs are primarily related to software used by clinics for operations and by the Company for the management of operations. Costs incurred in the preliminary stages of development are expensed as incurred. Once an application has reached the development stage, internal and external costs, if direct, are capitalized as assets in progress until the software is substantially complete and ready for its intended use. Capitalization ceases upon completion of all substantial testing. The Company also capitalizes costs related to specific upgrades and enhancements when it is probable the expenditures will result in additional functionality. Software developed is recorded as part of property and equipment. Maintenance and training costs are expensed as incurred. Internal use software is amortized on a straight-line basis over its estimated useful life, which is generally five years.
Leases
The Company adopted the guidance of Accounting Standards Codification 842 – Leases (“ASC 842”) on January 1, 2019 which requires lessees to recognize a right-of-use ("ROU") asset and lease liability for all leases. The Company elected the package of transition practical expedients for existing contracts, which allowed the Company to carry forward its historical assessments of whether contracts are or contain leases, lease classification and determination of initial direct costs.
The Company leases property and equipment under operating and finance leases. The Company leases its corporate office space and the space for each of the company-owned or managed clinic in the portfolio. Determining the lease term and amount of lease payments to include in the calculation of the ROU asset and lease liability for leases containing options requires the use of judgment to determine whether the exercise of an option is reasonably certain and if the optional period and payments should be included in the calculation of the associated ROU asset and liability. In making this determination, all relevant economic factors are considered that would compel the Company to exercise or not exercise an option. When available, the Company uses the rate implicit in the lease to discount lease payments; however, the rate implicit in the lease is not readily determinable for substantially all of its leases. In such cases, the Company estimates its incremental borrowing rate as the interest rate it would pay to borrow an amount equal to the lease payments over a similar term, with similar collateral as in the lease, and in a similar economic environment. The Company estimates these rates using available evidence such as rates imposed by third-party lenders to the Company in recent financings or observable risk-free interest rate and credit spreads for commercial debt of a similar duration, with credit spreads correlating to the Company’s estimated creditworthiness.
For operating leases that include rent holidays and rent escalation clauses, the Company recognizes lease expense on a straight-line basis over the lease term from the date it takes possession of the leased property. Pre-opening costs are recorded as incurred in general and administrative expenses. The Company records the straight-line lease expense and any contingent rent, if applicable, in general and administrative expenses on the consolidated statements of operations. Many of the Company’s leases also require it to pay real estate taxes, common area maintenance costs and other occupancy costs which are also included in general and administrative expenses on the consolidated statements of operations.
Intangible Assets
Intangible assets consist primarily of re-acquired franchise and regional developer rights and customer relationships. The Company amortizes the fair value of re-acquired franchise rights over the remaining contractual terms of the re-acquired franchise rights at the time of the acquisition, which generally range from three to eight years. In the case of regional developer rights, the Company generally amortizes the re-acquired regional developer rights over seven years. The fair value of customer relationships is amortized over their estimated useful life of two years.
Goodwill
Goodwill consists of the excess of the purchase price over the fair value of tangible and identifiable intangible assets acquired in the acquisitions of franchises. Goodwill and intangible assets deemed to have indefinite lives are not amortized but are subject to annual impairment tests. As required, the Company performs an annual impairment test of goodwill as of the first day of the fourth quarter or more frequently if events or circumstances change that would more likely than not reduce the fair value of a reporting unit below its carrying value. No impairments of goodwill were recorded for the years ended December 31, 2019 and 2018.
Long-Lived Assets
The Company reviews its long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying amount of the asset may not be recovered. The Company looks primarily to estimated undiscounted future cash flows in its assessment of whether or not long-lived assets are recoverable. No impairments of long-lived assets were recorded for the year ended December 31, 2019. The Company recorded an impairment of approximately $343,000 in long-lived assets for the year ended December 31, 2018.
Advertising Fund
The Company has established an advertising fund for national/regional marketing and advertising of services offered by its clinics. The monthly marketing fee is 2% of clinic sales. The Company segregates the marketing funds collected which are included in restricted cash on its consolidated balance sheets. As amounts are expended from the fund, the Company recognizes a related expense.
Co-Op Marketing Funds
Some franchises have established regional Co-Ops for advertising within their local and regional markets. The Company maintains a custodial relationship under which the marketing funds collected are segregated and used for the purposes specified by the Co-Ops’ officers. The marketing funds are included in restricted cash on the Company’s consolidated balance sheets.
Revenue Recognition
The Company generates revenue primarily through its company-owned and managed clinics, royalties, franchise fees, advertising fund, and through IT related income and computer software fees.
Revenues from Company-Owned or Managed Clinics. The Company earns revenues from clinics that it owns and operates or manages throughout the United States. In those states where the Company owns and operates or manages the clinic, revenues are recognized when services are performed. The Company offers a variety of membership and wellness packages which feature discounted pricing as compared with its single-visit pricing. Amounts collected in advance for membership and wellness packages are recorded as deferred revenue and recognized when the service is performed. The Company recognizes a contract liability (or a deferred revenue liability) related to the prepaid treatment plans for which the Company has an ongoing performance obligation. The Company recognizes this contract liability, and recognizes revenue, as the patient consumes his or her visits related to the package and the Company transfers its services. Based on a historical lag analysis and an evaluation of legal obligation by jurisdiction, the Company concluded that any remaining contract liability that exists after 12 to 24 months from transaction date will be deemed breakage. Breakage revenue is recognized only at that point, when the likelihood of the patient exercising his or her remaining rights becomes remote.
Royalties and Advertising Fund Revenue. The Company collects royalties, as stipulated in the franchise agreement, equal to 7% of gross sales, and a marketing and advertising fee currently equal to 2% of gross sales. Royalties, including franchisee contributions to advertising funds, are calculated as a percentage of clinic sales over the term of the franchise agreement. The franchise agreement royalties, inclusive of advertising fund contributions, represent sales-based royalties that are related entirely to the Company’s performance obligation under the franchise agreement and are recognized as franchisee clinic level sales occur. Royalties are collected bi-monthly two working days after each sales period has ended.
Franchise Fees. The Company requires the entire non-refundable initial franchise fee to be paid upon execution of a franchise agreement, which typically has an initial term of ten years. Initial franchise fees are recognized ratably on a straight-line basis over the term of the franchise agreement. The Company’s services under the franchise agreement include: training of franchisees and staff, site selection, construction/vendor management and ongoing operations support. The Company provides no financing to franchisees and offers no guarantees on their behalf. The services provided by the Company are highly interrelated with the franchise license and as such are considered to represent a single performance obligation.
Software Fees. The Company collects a monthly fee for use of its proprietary chiropractic software, computer support, and internet services support. These fees are recognized ratably on a straight-line basis over the term of the respective franchise agreement.
Regional Developer Fees. During 2011, the Company established a regional developer program to engage independent contractors to assist in developing specified geographical regions. Under the historical program, regional developers paid a license fee for each franchise they received the right to develop within the region. In 2017, the program was revised to grant exclusive geographical territory and establish a minimum development obligation within that defined territory. Regional developer fees paid to the Company are non-refundable and are recognized as revenue ratably on a straight-line basis over the term of the regional developer agreement, which is considered to begin upon the execution of the agreement. The Company’s services under regional developer agreements include site selection, grand opening support for the clinics, sales support for identification of qualified franchisees, general operational support and marketing support to advertise for ownership opportunities. The services provided by the Company are highly interrelated with the development of the territory and the resulting franchise licenses sold by the regional developer and as such are considered to represent a single
performance obligation. In addition, regional developers receive fees which are funded by the initial franchise fees collected from franchisees upon the sale of franchises within their exclusive geographical territory and a royalty of 3% of sales generated by franchised clinics in their exclusive geographical territory. Fees related to the sale of franchises within their exclusive geographical territory are initially deferred as deferred franchise costs and are recognized as an expense in franchise cost of revenues when the respective revenue is recognized, which is generally over the term of the related franchise agreement. Royalties of 3% of sales generated by franchised clinics in their regions are also recognized as franchise cost of revenues as franchisee clinic level sales occur.
The Company entered into one regional developer agreement for the year ended December 31, 2019 and four regional developer agreements for the year ended December 31, 2018 for which it received approximately $0.3 million and $0.9 million, respectively, which was deferred as of the respective transaction dates and will be recognized as revenue ratably on a straight-line basis over the term of the regional developer agreement, which is considered to be upon the execution of the agreement. Certain of these regional developer agreements resulted in the regional developer acquiring the rights to existing royalty streams from clinics already open in the respective territory. In those instances, the revenue associated from the sale of the royalty stream is being recognized over the remaining life of the respective franchise agreements.
Advertising Costs
Advertising costs are expensed as incurred. Advertising expenses were $2,292,628 and $1,558,662, for years ended December 31, 2019 and 2018, respectively.
Income Taxes
Deferred income taxes are recognized for differences between the basis of assets and liabilities for financial statement and income tax purposes. The differences relate principally to depreciation of property and equipment and treatment of revenue for franchise fees and regional developer fees collected. Deferred tax assets and liabilities represent the future tax consequence for those differences, which will either be taxable or deductible when the assets and liabilities are recovered or settled. Deferred taxes are also recognized for operating losses that are available to offset future taxable income. Valuation allowances are established when necessary to reduce deferred tax assets to the amount expected to be realized.
The Company accounts for uncertainty in income taxes by recognizing the tax benefit or expense from an uncertain tax position only if it is more likely than not that the tax position will be sustained upon examination by the taxing authorities, based on the technical merits of the position. The Company measures the tax benefits and expenses recognized in the consolidated financial statements from such a position based on the largest benefit that has a greater than 50% likelihood of being realized upon ultimate resolution. The Company has not identified any material uncertain tax positions as of December 31, 2019 and 2018, respectively. Interest and penalties associated with tax positions are recorded in the period assessed as general and administrative expenses.
With exceptions due to the generation and utilization of net operating losses or credits, as of December 31, 2019, the Company is no longer subject to federal and state examinations by taxing authorities for tax years before 2016 and 2015, respectively.
Earnings per Common Share
Basic earnings per common share is computed by dividing net income by the weighted-average number of common shares outstanding during the period. Diluted earnings per common share is computed by giving effect to all potentially dilutive common shares including restricted stock and stock options.
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| | | (as adjusted) |
| Net income | $ | 3,323,712 | | | $ | 146,696 | |
| | | |
| Weighted average common shares outstanding - basic | 13,819,149 | | | 13,669,107 | |
| Effect of dilutive securities: | | | |
| Unvested restricted stock and stock options | 648,418 | | | 362,610 | |
| Weighted average common shares outstanding - diluted | 14,467,567 | | | 14,031,717 | |
| | | |
| Basic earnings per share | $ | 0.24 | | | $ | 0.01 | |
| Diluted earnings per share | $ | 0.23 | | | $ | 0.01 | |
Potentially dilutive securities excluded from the calculation of diluted net income per common share as the effect would be anti-dilutive were as follows:
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| Unvested restricted stock | — | | | 6,896 | |
| Stock options | 39,286 | | | 236,205 | |
Stock-Based Compensation
The Company accounts for share-based payments by recognizing compensation expense based upon the estimated fair value of the awards on the date of grant. The Company determines the estimated grant-date fair value of restricted shares using the closing price on the date of the grant and the grant-date fair value of stock options using the Black-Scholes-Merton model. In order to calculate the fair value of the options, certain assumptions are made regarding the components of the model, including risk-free interest rate, volatility, expected dividend yield and expected option life. Changes to the assumptions could cause significant adjustments to the valuation. The Company recognizes compensation costs ratably over the period of service using the straight-line method. Forfeitures are estimated based on historical and forecasted turnover.
Retirement Benefit Plan
Employees of the Company are eligible to participate in a defined contribution retirement plan, the Joint Corp. 401(k) Retirement Plan (“401(k) Plan”), under Section 401(k) of the Internal Revenue Code. Under the 401(k) Plan, employees may contribute their eligible compensation, not to exceed the annual limits set by the IRS. The 401(k) Plan allows the Company to match participants’ contributions in an amount determined at the sole discretion of the Company. The Company matched participants’ contributions during fiscal years 2019 and 2018, up to a maximum of 2% of the employee’s eligible compensation. Employer contributions totaled $103,745 and $61,157, for fiscal years 2019 and 2018, respectively.
Use of Estimates
The preparation of the consolidated financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. Actual results could differ from those estimates. Items subject to significant estimates and assumptions include the allowance for doubtful accounts, share-based compensation arrangements, fair value of stock options, useful lives and realizability of long-lived assets, classification of deferred revenue and revenue recognition related to breakage, classification of deferred franchise costs, calculation of ROU assets and liabilities related to leases, realizability of deferred tax assets, impairment of goodwill and intangible assets and purchase price allocations and related valuation.
Recent Accounting Pronouncements
Recently Adopted Accounting Guidance
On January 1, 2019, the Company adopted ASC 842, which requires lessees to recognize a ROU asset and lease liability on their balance sheet for all leases with terms beyond twelve months. The new standard also requires enhanced disclosures that provide more transparency and information to financial statement users about lease portfolios. Effective January 1, 2019, the Company adopted the requirements of ASC 842 using the modified retrospective approach using the optional transition method and elected to apply the provisions of the standard as of the adoption date rather than the earliest date presented. The consolidated financial statements for the period ended December 31, 2019 are presented under the new standard, while comparative periods presented have not been adjusted and continue to be reported in accordance with the previous standard.
During the process of adoption, the Company made the following elections:
•The Company elected the package of practical expedients which allowed the Company to not reassess:
•Whether existing or expired contracts contain leases under the new definition of a lease;
•Lease classification for existing or expired leases; and
•Initial direct costs for any expired or existing leases to determine if they would qualify for capitalization under ASC 842.
•The Company did not elect the hindsight practical expedient, which permits the use of hindsight when determining lease term and impairment of operating lease assets.
•The Company did not elect the land easement practical expedient, which permits an entity to continue applying its current policy for accounting for land easements that existed as of, or expired before, the effective date of ASC 842.
•The Company elected to make the accounting policy election for short-term leases, permitting the Company to not apply the recognition requirements of ASC 842 to short-term leases with terms of 12 months or less.
The adoption of ASC 842 does not materially impact the Company’s results of operations other than recognition of the operating lease ROU asset and lease liability. See Note 12 for additional disclosures required by ASC 842.
Newly Issued Accounting Standards Not Yet Adopted
The Company reviewed other newly issued accounting pronouncements and concluded that they either are not applicable to the Company's operations or that no material effect is expected on the Company's financial statements upon future adoption.
Note 2: Acquisitions
On March 18, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which (i) the Company repurchased from the seller one operating franchise in West Covina, California and (ii) the parties agreed to terminate a second franchise agreement for an operating franchise. The Company operates the remaining franchise as a company-managed clinic. The total purchase price for the transaction was $30,000, less $3,847 of net deferred revenue resulting in total purchase consideration of $26,153.
On July 9, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which the Company repurchased from the seller one operating franchise in Phoenix, Arizona. The Company operates the franchise as a company-owned clinic. The total purchase price for the transaction was $400,000, less $9,835 of net deferred revenue resulting in total purchase consideration of $390,165.
On July 17, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which the Company repurchased from the seller three operating franchises in Savannah, Georgia, Pooler, Georgia and Bluffton, South Carolina. The Company operates the franchises as company-owned clinics. The total purchase price for the transaction was $1,604,918, less $13,449 of net deferred revenue resulting in total purchase consideration of $1,591,469.
On August 1, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which the Company repurchased from the seller one operating franchise in Sayebrook, South Carolina. The Company operates the franchise as a company-owned clinic. The total purchase price for the transaction was $727,414, less $5,236 of net deferred revenue resulting in total purchase consideration of $722,178.
On August 15, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which the Company repurchased from the seller one operating franchise in Chula Vista, California. The Company operates the franchise as a company-managed clinic. The total purchase price for the transaction was $310,000, less $4,328 of net deferred revenue resulting in total purchase consideration of $305,672.
On October 28, 2019, the Company entered into an Asset and Franchise Purchase Agreement under which the Company repurchased from the seller one operating franchise in Redlands, California. The Company operates the franchise as a company-managed clinic. The total purchase price for the transaction was $55,000, less $4,110 of net deferred revenue resulting in total purchase consideration of $50,890. As of December 31, 2019, $5,000 of remaining consideration was outstanding, which was paid in February 2020.
Purchase Price Allocation
The following summarizes the aggregate estimated fair values of the assets acquired and liabilities assumed during 2019 as of the acquisition date:
| | | | | |
| Property and equipment | $ | 173,521 | |
| Operating lease right-of-use asset | 1,283,608 | |
| Intangible assets | 1,999,469 | |
| Total assets acquired | 3,456,598 | |
| Goodwill | 925,315 | |
| Deferred revenue | (140,861) | |
| Operating lease liability - current portion | (256,601) | |
| Operating lease liability - net of current portion | (867,216) | |
| Deferred tax liability | (11,410) | |
| Bargain purchase gain | (19,298) | |
| Net purchase price | $ | 3,086,527 | |
Intangible assets in the table above consist of reacquired franchise rights of $1,488,494 amortized over an estimated useful life of approximately three years and customer relationships of $510,975 amortized over an estimated useful life of two years.
Goodwill was established due primarily to synergies and benefits expected to be gained from leveraging the Company’s existing operations and infrastructures, as well as the expected associated revenue and cash flow projections. Goodwill has been allocated to the Company’s Corporate Clinics segment based on such expected benefits. Goodwill related to the acquisitions is expected to be deductible for income tax purposes over the next 15 years. The purchase price allocations are preliminary, and the Company expects to finalize the allocations during fiscal year 2020.
Pro Forma Results of Operations (Unaudited)
The following table summarizes selected unaudited pro forma consolidated statements of operations data for the years ended December 31, 2019 and 2018 as if the acquisition in 2019 had been completed on January 1, 2018.
| | | | | | | | | | | |
| Pro Forma for the Year Ended | | |
| December 31, 2019 | | December 31, 2018 |
| Revenues, net | $ | 50,399,700 | | | $ | 39,774,609 | |
| Net income (loss) | $ | 3,241,918 | | | $ | (77,662) | |
This selected unaudited pro forma consolidated financial data is included only for the purpose of illustration and does not necessarily indicate what the operating results would have been if the acquisition had been completed on that date. Moreover, this information is not indicative of what the Company’s future operating results will be. The information for 2018 and 2019 prior to the acquisitions is included based on prior accounting records maintained by the acquired companies. In some cases, accounting policies differed materially from accounting policies adopted by the Company following the acquisitions. For 2019, this information includes actual data recorded in the Company’s financial statements for the period subsequent to the date of the acquisition. The Company’s consolidated statement of operations for the year ended December 31, 2019 includes net revenue and net income of approximately $1,529,000 and $218,000, respectively, attributable to the acquisitions.
The pro forma amounts included in the table above reflect the application of accounting policies and adjustment of the results of the clinics to reflect the additional depreciation and amortization that would have been charged assuming the fair value adjustments to property and equipment and intangible assets had been applied from January 1, 2018. The pro forma earnings do not include adjustments related to acquisition-related costs incurred in 2019, which were not material.
Note 3: Revenue Disclosures
Company-owned or Managed Clinics
The Company earns revenues from clinics that it owns and operates or manages throughout the United States. Revenues are recognized when services are performed. The Company offers a variety of membership and wellness packages which feature discounted pricing as compared with its single-visit pricing. Amounts collected in advance for membership and wellness packages are recorded as deferred revenue and recognized when the service is performed or in accordance with the Company’s breakage policy as discussed in Note 1, Revenue Recognition.
Franchising Fees, Royalty Fees, Advertising Fund Revenue, and Software Fees
The Company currently franchises its concept across 33 states. The franchise arrangement is documented in the form of a franchise agreement. The franchise arrangement requires the Company to perform various activities to support the brand that do not directly transfer goods and services to the franchisee, but instead represent a single performance obligation, which is the transfer of the franchise license. The intellectual property subject to the franchise license is symbolic intellectual property as it does not have significant standalone functionality, and substantially all of the utility is derived from its association with the Company’s past or ongoing activities. The nature of the Company’s promise in granting the franchise license is to provide the franchisee with access to the brand’s symbolic intellectual property over the term of the license. The services provided by the Company are highly interrelated with the franchise license and as such are considered to represent a single performance obligation.
The transaction price in a standard franchise arrangement primarily consists of (a) initial franchise fees; (b) continuing franchise fees (royalties); (c) advertising fees; and (d) software fees. Since the Company considers the licensing of the franchising right to be a single performance obligation, no allocation of the transaction price is required.
The Company recognizes the primary components of the transaction price as follows:
•Franchise fees are recognized as revenue ratably on a straight-line basis over the term of the franchise agreement commencing with the execution of the franchise agreement. As these fees are typically received in cash at or near the beginning of the franchise term, the cash received is initially recorded as a contract liability until recognized as revenue over time;
•The Company is entitled to royalties and advertising fees based on a percentage of the franchisee's gross sales as defined in the franchise agreement. Royalty and advertising revenue are recognized when the franchisee's sales occur. Depending on timing within a fiscal period, the recognition of revenue results in either what is considered a contract asset (unbilled receivable) or, once billed, accounts receivable, on the balance sheet.
•The Company is entitled to a software fee, which is charged monthly. The Company recognizes revenue related to software fees ratably on a straight-line basis over the term of the franchise agreement.
In determining the amount and timing of revenue from contracts with customers, the Company exercises significant judgment with respect to collectability of the amount; however, the timing of recognition does not require significant judgment as it is based on either the franchise term or the reported sales of the franchisee, none of which require estimation. The Company believes its franchising arrangements do not contain a significant financing component.
The Company recognizes advertising fees received under franchise agreements as advertising fund revenue.
Regional Developer Fees
The Company currently utilizes regional developers to assist in the development of the brand across certain geographic territories. The arrangement is documented in the form of a regional developer agreement. The arrangement between the Company and the regional developer requires the Company to perform various activities to support the brand that do not directly transfer goods and services to the regional developer, but instead represent a single performance obligation, which is the transfer of the development rights to the defined geographic region. The intellectual property subject to the development rights is symbolic intellectual property as it does not have significant standalone functionality, and substantially all of the utility is derived from its association with the Company’s past or ongoing activities. The nature of the Company’s promise in granting the development rights is to provide the regional developer with access to the brand’s symbolic intellectual property over the term of the agreement. The services provided by the Company are highly interrelated with the development of the territory and the resulting franchise licenses sold by the regional developer and as such are considered to represent a single performance obligation.
The transaction price in a standard regional developer arrangement primarily consists of the initial territory fees. The Company recognizes the regional developer fee as revenue ratably on a straight-line basis over the term of the regional developer agreement commencing with the execution of the regional developer agreement. As these fees are typically received in cash at or near the beginning of the term of the regional developer agreement, the cash received is initially recorded as a contract liability until recognized as revenue over time.
Disaggregation of Revenue
The Company believes that the captions contained on the consolidated statements of operations appropriately reflect the disaggregation of its revenue by major type for the years ended December 31, 2019 and 2018. Other revenues primarily consist of merchant income associated with credit card transactions.
Rollforward of Contract Liabilities and Contract Assets
Changes in the Company's contract liability for deferred franchise and regional development fees during the year ended December 31, 2019 and 2018 were as follows (in thousands):
| | | | | |
| Deferred Revenue
short and long-term |
| Balance at December 31, 2017 | $ | 11,547 | |
| Recognized as revenue during the year ended December 31, 2018 | (2,287) | |
| Fees received and deferred during the year ended December 31, 2018 | 4,349 | |
| Balance at December 31, 2018 | $ | 13,609 | |
| Recognized as revenue during the year ended December 31, 2019 | (2,595) | |
| Fees received and deferred, net | 4,093 | |
| Balance at December 31, 2019 | $ | 15,107 | |
Changes in the Company's contract assets for deferred franchise costs during the year ended December 31, 2019 and 2018 were as follows (in thousands):
| | | | | |
| Deferred Franchise Costs short and long-term |
| Balance at December 31, 2017 | $ | 2,811 | |
| Recognized as cost of revenue during the year ended December 31, 2018 | (631) | |
| Costs incurred and deferred during the year ended December 31, 2018 | 1,309 | |
| Balance at December 31, 2018 | $ | 3,489 | |
| Recognized as cost of revenue during the year ended December 31, 2019 | (812) | |
| Costs incurred and deferred, net | 1,716 | |
| Balance at December 31, 2019 | $ | 4,393 | |
The following table illustrates revenues expected to be recognized in the future related to performance obligations that were unsatisfied (or partially unsatisfied) as of December 31, 2019 (in thousands):
| | | | | |
| Contract liabilities expected to be recognized in | Amount |
| 2020 | $ | 2,741 | |
| 2021 | 2,626 | |
| 2022 | 2,240 | |
| 2023 | 1,907 | |
| 2024 | 1,477 | |
| Thereafter | 4,116 | |
| Total | $ | 15,107 | |
Note 4: Restricted Cash
The table below reconciles the cash and cash equivalents balance and restricted cash balances from the Company’s consolidated balance sheets to the amount of cash reported on the consolidated statements of cash flows:
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| Cash and cash equivalents | $ | 8,455,989 | | | $ | 8,716,874 | |
| Restricted cash | 185,888 | | | 138,078 | |
| Total cash, cash equivalents and restricted cash | $ | 8,641,877 | | | $ | 8,854,952 | |
Note 5: Notes Receivable
Effective April 29, 2017, the Company entered into a regional developer agreement for certain territories in the state of Florida in exchange for $320,000, of which $187,000 was funded through a promissory note. The note bears interest at 10% per annum for 42 months and requires monthly principal and interest payments over 36 months, beginning November 1, 2017 and maturing on October 1, 2020. The note is secured by the regional developer rights in the respective territory.
Effective August 31, 2017, the Company entered into a regional developer agreement for certain territories in Maryland/Washington DC in exchange for $220,000, of which $117,475 was funded through a promissory note. The note bears interest at 10% per annum for 36 months and requires monthly principal and interest payments over 36 months, beginning September 1, 2017 and maturing on August 1, 2020. The note is secured by the regional developer rights in the respective territory.
Effective September 22, 2017, the Company entered into a regional developer and asset purchase agreement for certain territories in Minnesota in exchange for $228,293, of which $119,147 was funded through a promissory note. The note bears interest at 10% per annum for 36 months and requires monthly principal and interest payments over 36 months, beginning October 1, 2017 and maturing on September 1, 2020. The note was secured by the regional developer rights in the territory. The note was paid in full on September 28, 2018.
Effective October 10, 2017, the Company entered into a regional developer agreement for certain territories in Texas, Oklahoma and Arkansas in exchange for $170,000, of which $135,688 was funded through a promissory note. The note bears interest at 10% per annum for 36 months and requires monthly principal and interest payments over 36 months, maturing on October 24, 2020. The note is secured by the regional developer rights in the territory.
Effective April 26, 2019, the Company entered into a promissory note valued at $31,086. The note bears interest at 0% per annum for 36 months and requires monthly principal payments over 36 months, beginning May 15, 2019 and maturing on May 15, 2022.
The net outstanding balances of the notes as of December 31, 2019, and 2018 were $155,810 and $278,072, respectively. Allowance reserve on the outstanding notes as of December 31, 2019 was $27,086. Maturities of notes receivable as of December 31, 2019 are as follows:
| | | | | |
| 2020 | $ | 137,124 | |
| 2021 | 9,600 | |
| 2022 | $ | 9,086 | |
| Total | $ | 155,810 | |
Note 6: Property and Equipment
Property and equipment consist of the following:
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| Office and computer equipment | $ | 1,594,364 | | | $ | 1,243,104 | |
| Leasehold improvements | 7,154,156 | | | 5,407,915 | |
| Software developed | 1,193,007 | | | 1,145,742 | |
| Finance lease assets | 80,604 | | | — | |
| 10,022,131 | | | 7,796,761 | |
| Accumulated depreciation and amortization | (5,671,366) | | | (4,909,002) | |
| 4,350,765 | | | 2,887,759 | |
| Construction in progress | 2,230,823 | | | 770,248 | |
| Property and Equipment, net | $ | 6,581,588 | | | $ | 3,658,007 | |
Depreciation expense was $823,679 and $1,049,942 for the years ended December 31, 2019 and 2018, respectively.
Amortization expense related to finance lease assets was $24,675 for the year ended December 31, 2019.
Construction in progress at December 31, 2019 and 2018 principally relate to development costs for a software to be used by clinics for operations and by the Company for the management of operations.
In August 2018, the Board of Directors approved a change in strategy as it relates to the development of the Company’s IT platform. The Company ceased its related internal development, and as a result, the Company recorded an impairment of approximately $343,000 of previously capitalized software development costs during the year ended December 31, 2018.
Note 7: Fair Value Consideration
The Company’s financial instruments include cash, restricted cash, accounts receivable, notes receivable, accounts payable, accrued expenses and notes payable. The carrying amounts of its financial instruments approximate their fair value due to their short maturities.
The Company does not use derivative financial instruments to hedge exposures to cash-flow, market or foreign-currency risks.
Authoritative guidance defines fair value as the price that would be received to sell an asset or paid to transfer a liability (an exit price) in an orderly transaction between market participants at the measurement date. The guidance establishes a hierarchy for inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the most observable inputs be used when available. Observable inputs are inputs that market participants would use in pricing the asset or liability, developed based on market data obtained from sources independent of the Company. Unobservable inputs are inputs that reflect the Company’s assumptions of what market participants would use in pricing the asset or liability developed based on the best information available in the circumstances. The hierarchy is broken down into three levels based on reliability of the inputs as follows:
Level 1: Observable inputs such as quoted prices in active markets;
Level 2: Inputs, other than the quoted prices in active markets, that are observable either directly or indirectly; and
Level 3: Unobservable inputs in which there is little or no market data, which require the reporting entity to develop its own assumptions.
As of December 31, 2019, and 2018, the Company did not have any financial instruments that are measured on a recurring basis as Level 1, 2 or 3.
The intangible assets resulting from the acquisitions (reference Note 2) were recorded at estimated fair value on a non-recurring basis and are considered Level 3 within the fair value hierarchy.
Note 8: Intangible Assets and Goodwill
On February 4, 2019, the Company entered into an agreement under which it repurchased the right to develop franchises in various counties in South Carolina and Georgia. The total consideration for the transaction was $681,500. The Company carried a deferred revenue balance associated with these transactions of $44,334, representing unrecognized portion of the license fees collected upon the execution of the regional developer agreements. The Company accounted for the termination of development rights associated with unsold or undeveloped franchises as a cancellation, and the associated deferred revenue was netted against the aggregate purchase price.
Intangible assets consisted of the following:
| | | | | | | | | | | | | | | | | |
| December 31, 2019 | | | | |
| Gross Carrying Amount | | Accumulated Amortization | | Net Carrying Value |
| Intangible assets subject to amortization: | | | | | |
| Reacquired franchise rights | $ | 3,246,494 | | | $ | 1,400,086 | | | $ | 1,846,408 | |
| Customer relationships | 1,255,975 | | | 865,478 | | | 390,497 | |
| Reacquired development rights | 2,050,481 | | | 1,067,595 | | | 982,886 | |
| $ | 6,552,950 | | | $ | 3,333,159 | | | $ | 3,219,791 | |
| | | | | | | | | | | | | | | | | |
| December 31, 2018 | | | | |
| Gross Carrying Amount | | Accumulated Amortization | | Net Carrying Value |
| Intangible assets subject to amortization: | | | | | |
| Reacquired franchise rights | $ | 1,758,000 | | | $ | 921,138 | | | $ | 836,862 | |
| Customer relationships | 745,000 | | | 717,498 | | | 27,502 | |
| Reacquired development rights | 1,413,316 | | | 643,620 | | | 769,696 | |
| $ | 3,916,316 | | | $ | 2,282,256 | | | $ | 1,634,060 | |
Amortization expense related to the Company’s intangible assets was $1,050,903 and $506,298 for the years ended December 31, 2019 and 2018, respectively.
Estimated amortization expense for 2020 and subsequent years is as follows:
| | | | | |
| 2020 | $ | 1,409,962 | |
| 2021 | 1,212,703 | |
| 2022 | 539,750 | |
| 2023 | 57,376 | |
| |
| |
| Total | $ | 3,219,791 | |
The changes in the carrying amount of goodwill were as follows:
| | | | | | | | |
| | Corporate Clinic Segment |
| | |
| | |
| Balance as of December 31, 2018 | | | |
| Goodwill, gross | | $ | 3,280,139 | |
| Accumulated impairment losses | | (54,994) |
| Goodwill, net | | 3,225,145 | |
| 2019 acquisitions | | 925,316 |
| Balance as of December 31, 2019 | | | |
| Goodwill, gross | | 4,205,455 | |
| Accumulated impairment losses | | (54,994) | |
| Goodwill, net | | $ | 4,150,461 | |
There were no changes in the carrying amount of goodwill during the year ended December 31, 2018.
Note 9: Debt
Notes Payable
During 2016, the Company issued two notes payable totaling $186,000 as a portion of the consideration paid in connection with the Company’svarious acquisitions. Interest rates for both notes were 4.25% with maturities through May 2017. There was one outstanding note as of December 31, 2018 with a balance of $100,000 which was paid in February 2019.
Credit and Security Agreement
On January 3, 2017, the Company entered into a Credit and Security Agreement (the “Credit Agreement”) and signed a revolving credit note payable to the lender. Under the Credit Agreement, the Company was able to borrow up to an aggregate of $5,000,000 under revolving loans. Interest on the unpaid outstanding principal amount of any revolving loans was at a rate equal to 10% per annum, provided that the minimum amount of interest paid in the aggregate on all revolving loans granted over the term of the Credit Agreement is $200,000. Interest was due and payable on the last day of each fiscal quarter in an amount determined by the Company, but not less than $25,000. The Credit Agreement was collateralized by the assets in the Company’s company-owned or managed clinics. The Company used the credit facility for general working capital needs. During 2019, the Company had drawn $1,000,000 of the $5,000,000 available under the Credit Agreement which was repaid in full on December 20, 2019. The Credit Agreement was terminated in December 2019 in accordance with the provisions of the Credit Agreement. During 2019, the Company was in compliance with all applicable financial and non-financial covenants under the Credit Agreement. The Company recorded interest expense of $96,978 and $100,000 in the years ended December 31, 2019 and 2018 related to this Credit Agreement, respectively.
In February 2020, the Company executed a line of credit agreement which provides a credit facility up to $7,500,000, including a $2,000,000 revolver and $5,500,000 development line of credit. Please see Note 14, “Subsequent Events” in the Notes to Consolidated Financial Statements for further discussion.
Note 10: Stock-Based Compensation
The Company grants stock-based awards under its 2014 Incentive Stock Plan (the “2014 Plan”) and the 2012 Stock Plan (the “2012 Plan”). The 2014 Plan replaced the 2012 Plan, but the 2012 plan remains in effect for the administration of awards made prior to its replacement by the 2014 Plan. The shares issued as a result of stock-based compensation transactions generally have been funded with the issuance of new shares of the Company’s common stock.
The Company may grant the following types of incentive awards under the 2014 Plan: (i) non-qualified stock options; (ii) incentive stock options; (iii) stock appreciation rights; (iv) restricted stock; and (v) restricted stock units. Each award granted under the 2014 Plan is subject to an award agreement that incorporates, as applicable, the exercise price, the term of the award, the periods of restriction, the number of shares to which the award pertains, and such other terms and conditions as the plan committee determines. Awards granted under the 2014 Plan are classified as equity awards, which are recorded in stockholders’ equity in the Company’s Consolidated Balance Sheets.
Stock Options
The Company’s closing price on the date of grant is the basis of fair value of its common stock used in determining the value of share-based awards. To the extent the value of the Company’s share-based awards involves a measure of volatility, the Company historically relied on the volatilities from publicly-traded companies with similar business models as its common stock lacked enough trading history for it to utilize its own historical volatility. Effective July 1, 2019, the Company uses available historical volatility of the Company’s common stock over a period of time corresponding to the expected stock option term. The Company uses the simplified method to calculate the expected term of stock option grants to employees as the Company does not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term of stock options granted to employees. Accordingly, the expected life of the options granted is based on the average of the vesting term, which is generally four years and the contractual term, which is generally ten years. The Company will continue to evaluate the appropriateness of utilizing such method. The risk-free interest rate is based on United States Treasury yields in effect at the date of grant for periods corresponding to the expected stock option term.
The Company has computed the fair value of all options granted using the Black-Scholes-Merton model during the years ended December 31, 2019 and 2018, using the following assumptions:
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| Expected volatility | 35% to 55% | | 35% | |
| Expected dividends | None | | | None | |
| Expected term (years) | 7 | | 7 |
| Risk-free rate | 1.89% to 2.61% | | 2.53% to 2.90% |
| Forfeiture rate | 20% | | | 20% | |
The information below summarizes the stock options:
| | | | | | | | | | | | | | | | | |
| Number of
Shares | | Weighted
Average
Exercise
Price | | Weighted
Average
Remaining
Contractual Life |
| Outstanding at December 31, 2017 | 1,003,916 | | | $ | 4.18 | | | 8.1 |
| Granted at market price | 145,792 | | | 7.00 | | | |
| Exercised | (95,162) | | | 3.48 | | | |
| Cancelled | (67,855) | | | 3.37 | | | |
| Outstanding at December 31, 2018 | 986,691 | | | $ | 4.72 | | | 6.8 |
| Granted at market price | 65,759 | | | 12.31 | | | |
| Exercised | (103,205) | | | 5.28 | | | |
| Cancelled | — | | | — | | | |
| Outstanding at December 31, 2019 | 949,245 | | | $ | 5.19 | | | 6.5 |
| Exercisable at December 31, 2019 | 592,265 | | | $ | 4.54 | | | 5.9 |
The aggregate intrinsic value of the Company's stock options exercised during 2019 and 2018 was $1,236,099 and $412,952, respectively.
The aggregate intrinsic value of the Company’s stock options outstanding and expected to vest was $9,788,395 at December 31, 2019.
The aggregate intrinsic value of the Company’s stock options exercisable was $6,872,930 at December 31, 2019.
The weighted-average grant-date fair value of the Company's stock options granted during 2019 and 2018 was $5.21 and $2.95, respectively.
The aggregate fair value of the Company's stock options vested during 2019 and 2018 was $388,672 and $509,729, respectively.
For the years ended December 31, 2019 and 2018, stock-based compensation expense for stock options was $418,301 and $363,568, respectively.
Unrecognized stock-based compensation expense for stock options as of December 31, 2019 was $729,263, which is expected to be recognized ratably over the next 2.5 years.
Restricted Stock
Restricted stock awards granted to employees generally vest in four equal annual installments. Restricted stock awards granted to non-employee directors vest on the earlier of (i) one year from the grant date and (ii) the date of the next annual meeting of the shareholders of the Company occurring after the date of grant.
The information below summaries the restricted stock activity:
| | | | | | | | | | | |
| Restricted Stock Awards | Shares | | Weighted Average Grant-Date Fair Value per Award |
| Non-vested at December 31, 2018 | 51,134 | | | $ | 7.64 | |
| Granted | 26,131 | | | $ | 14.30 | |
| Vested | (38,289) | | | $ | 7.44 | |
| Cancelled | — | | | $ | — | |
| Non-vested at December 31, 2019 | 38,976 | | | $ | 12.31 | |
For the years ended December 31, 2019 and 2018, stock-based compensation expense for restricted stock was $302,350 and $264,862, respectively. Unrecognized stock-based compensation expense for restricted stock awards as of December 31, 2019 was $321,031 to be recognized ratably over 2.1 years.
Warrants
In conjunction with the IPO, the Company issued warrants to the underwriters for the purchase of 90,000 shares of common stock, which were exercisable between November 10, 2015 and November 10, 2018 at an exercise price of $8.125 per share. The fair value of the warrants was determined using the Black-Scholes-Merton option valuation model. The unexercised warrants expired on November 10, 2018.
Note 11: Income Taxes
Income tax provision (benefit) reported in the consolidated statements of operations is comprised of the following (rounded to hundreds):
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| Current provision (benefit): | | | |
| Federal | $ | — | | | $ | — | |
| State, net of state tax credits | 47,200 | | | 39,300 | |
| Total current provision (benefit) | 47,200 | | | 39,300 | |
| Deferred provision (benefit): | | | |
| Federal | 800 | | | (90,000) | |
| State | 1,000 | | | 13,000 | |
| Total deferred provision (benefit) | 1,800 | | | (77,000) | |
| Total income tax provision (benefit) | $ | 49,000 | | | $ | (37,700) | |
The following are the components of the Company’s deferred tax assets (liabilities) for federal and state income taxes (rounded to hundreds):
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| | | (as adjusted) | |
| Deferred income tax assets: | | | | |
| Accrued expenses | $ | 515,800 | | | $ | 361,100 | |
| Deferred revenue | 4,435,400 | | | 3,092,500 | |
| Deferred rent | — | | | 237,900 | |
| Lease abandonment | — | | | 96,500 | |
| Lease liability | 3,782,800 | | | — | |
| Goodwill - component 2 | 55,300 | | | 52,500 | |
| Restricted stock compensation | 3,900 | | | — | |
| Nonqualified stock options | 198,900 | | | 184,400 | |
| Net operating loss carryforwards | 3,585,700 | | | 6,175,600 | |
| Tax credits | 33,800 | | | 14,000 | |
| Charitable contribution carryover | — | | | 15,500 | |
| Asset basis difference related to property and equipment | 214,000 | | | 458,600 | |
| Intangibles | 595,800 | | | 435,900 | |
| Total deferred income tax assets | 13,421,400 | | | 11,124,500 | |
| Deferred income tax liabilities: | | | | | |
| Lease right-of-use asset | (3,267,900) | | | — | |
| Deferred franchise costs | (406,500) | | | (574,100) | |
| Goodwill - component 1 | (245,500) | | | (194,700) | |
| Restricted stock compensation | — | | | (30,800) | |
| Total deferred income tax liabilities | (3,919,900) | | | (799,600) | |
| Valuation allowance | (9,591,400) | | | (10,401,600) | |
| Net deferred tax liability | $ | (89,900) | | | $ | (76,700) | |
Management assesses the available positive and negative evidence to estimate whether sufficient future taxable income will be generated to permit use of the existing deferred tax assets. A significant piece of objective negative evidence evaluated was the lack of sustained profitability over the three-year period ended December 31, 2019. Such objective evidence limits the ability to consider other subjective evidence, such as the Company's projections for future growth. On the basis of this evaluation, as of December 31, 2019, a valuation allowance of $9,591,400 has been recorded to recognize only the portion of the deferred tax asset that is more likely than not to be realized. The amount of the deferred tax asset considered realizable, however, could be adjusted if estimates of future taxable income during the carryforward period are reduced or increased or if objective negative evidence in the form of cumulative losses is no longer present and additional weight is given to subjective evidence such as the Company's projections for growth. If and when the Company determines the valuation allowance should be released (i.e., reduced), the adjustment would result in a tax benefit reported in that period’s consolidated statement of operations, the effect of which would be an increase in reported net income. The amount of any such tax benefit associated with release of the Company's valuation allowance in a particular reporting period may be material.
The 2017 Tax Act was signed into law on December 22, 2017. The 2017 Tax Act significantly revises the U.S. corporate income tax by, among other things, lowering the statutory corporate tax rate from 34% to 21%, eliminating certain deductions, imposing a mandatory one-time tax on accumulated earnings of foreign subsidiaries, introducing new tax regimes, and changing how foreign earnings are subject to U.S. tax. The Company finalized the effects of the 2017 Tax Act and recorded the impact in its financial statements as of December 22, 2018 under Staff Accounting Bulletin No. 118 (SAB 118). The company recorded a tax benefit for the impact of the 2017 Tax Act of approximately $120,000 in 2018. This amount is a remeasurement of federal net deferred tax assets resulting from the permanent reduction in the U.S. statutory corporate tax rate to 21% from 34%.
At December 31, 2019, The Joint Corp., without the VIE, had federal and state net operating losses of approximately $13,262,000 and $17,728,000, respectively. These net operating losses are available to offset future taxable income and will begin to expire in 2035 for federal purposes and 2025 for state purposes. The Joint Corp. has research and development credits of $14,000 that will begin to expire in 2031 and $20,000 California alternative minimum tax credits that do not expire.
The following is a reconciliation of the statutory federal income tax rate applied to pre-tax accounting net income, compared to the income tax provision (benefit) in the consolidated statement of operations (rounded to hundreds):
| | | | | | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, | | | | | | |
| | 2019 | | | | 2018 (as adjusted) | | |
| | Amount | | Percent | | Amount | | Percent |
| Expected federal tax expense (benefit) | $ | 731,600 | | | 21.0 | % | | $ | 22,900 | | | 21.0 | % |
| State tax provision, net of federal benefit | 315,800 | | | 9.1 | % | | (63,600) | | | (58.4) | % |
| Change in valuation allowance | (810,200) | | | (23.3) | % | | 51,600 | | | 47.4 | % |
| Other permanent differences | 41,700 | | | 1.2 | % | | 13,200 | | | 12.1 | % |
| Stock compensation | (232,600) | | | (6.7) | % | | (40,800) | | | (37.4) | % |
| Bargain purchase gain | (5,100) | | | (0.1) | % | | (16,100) | | | (14.8) | % |
| Return to provision adjustments | 7,800 | | | 0.2 | % | | (4,900) | | | (4.5) | % |
| Provision (benefit) | $ | 49,000 | | | 1.4 | % | | $ | (37,700) | | | (34.6) | % |
Changes in the Company's income tax expense relate primarily to changes in pretax income during the year ended December 31, 2019, as compared to year ended December 31, 2018, and the effective tax rate was 1.4% and (34.6)%, respectively. For the years ended December 31, 2019 and December 31, 2018, the difference between the statutory federal income tax rate and the Company's effective tax rate was primarily due to state taxes, the valuation allowance, VIE permanent differences, and stock-based compensation.
For the years ended December 31, 2019 and December 31, 2018, the Company had no uncertain tax positions or interest and penalties related to uncertain tax positions. Interest and penalties associated with tax positions are recorded in the period assessed as general and administrative expenses, if any.
With exceptions due to the generation and utilization of net operating losses or credits, as of December 31, 2019, the Company is no longer subject to federal and state examinations by taxing authorities for tax years before 2016 and 2015, respectively.
Note 12: Commitments and Contingencies
Operating Leases
The table below summarizes the components of lease expense and income statement location for the year ended December 31, 2019:
| | | | | | | | | | | |
| Line Item in the Company’s Consolidated Statements of Operations | | Year Ended December 31, 2019 |
| Finance lease costs: | | | |
| Amortization of assets | Depreciation and amortization | | $ | 24,675 | |
| Interest on lease liabilities | Other expense, net | | 6,832 | |
| Total finance lease costs | | | $ | 31,507 | |
| Operating lease costs | General and administrative expenses | | $ | 3,005,124 | |
| Total lease costs | | | $ | 3,036,631 | |
Supplemental information and balance sheet location related to leases is as follows:
| | | | | |
| December 31, 2019 |
| Operating Leases: | |
| Operating lease right-of -use asset | $ | 12,486,672 | |
| Operating lease liability - current portion | 2,313,109 | |
| Operating lease liability - net of current portion | 11,901,040 | |
| Total operating lease liability | $ | 14,214,149 | |
| Finance Leases: | |
| Property and equipment, at cost | 80,604 | |
| Less accumulated amortization | (24,675) | |
| Property and equipment, net | $ | 55,929 | |
| |
| Finance lease liability - current portion | 24,253 | |
| Finance lease liability - net of current portion | 34,398 | |
| Total finance lease liabilities | $ | 58,651 | |
| |
| Weighted average remaining lease term (in years): | |
| Operating leases | 5.4 |
| Finance lease | 2.3 |
| |
| Weighted average discount rate: | |
| Operating leases | 8.7 | % |
| Finance leases | 10.0 | % |
Supplemental cash flow information related to leases is as follows:
| | | | | |
| Year Ended December 31, 2019 |
| |
| Cash paid for amounts included in measurement of liabilities: | |
| Operating cash flows from operating leases | $ | 2,834,903 | |
| Operating cash flows from finance leases | 6,832 | |
| Financing cash flows from finance leases | 21,954 | |
| |
| Non-cash transactions: ROU assets obtained in exchange for lease liabilities | |
| Operating lease | $ | 1,350,090 | |
| Finance lease | 80,604 | |
Maturities of lease liabilities as of December 31, 2019 are as follows:
| | | | | | | | | | | |
| Operating Leases | | Finance Lease |
| 2020 | $ | 3,376,830 | | | $ | 28,786 | |
| 2021 | 3,545,186 | | | 28,786 | |
| 2022 | 3,430,110 | | | 7,676 | |
| 2023 | 2,716,465 | | | — | |
| 2024 | 2,096,333 | | | — | |
| Thereafter | 2,629,450 | | | — | |
| Total lease payments | 17,794,374 | | | 65,248 | |
| Less: Imputed interest | (3,580,225) | | | (6,597) | |
| Total lease obligations | 14,214,149 | | | 58,651 | |
| Less: Current obligations | (2,313,109) | | | (24,253) | |
| Long-term lease obligation | $ | 11,901,040 | | | $ | 34,398 | |
The future minimum obligations under operating leases in effect as of December 31, 2018 having a noncancelable term in excess of one year as determined prior to the adoption of ASC 842 are as follows:
| | | | | |
| Operating Leases | |
| 2020 | $ | 2,630,443 | |
| 2021 | 2,406,645 | |
| 2022 | 2,299,887 | |
| 2023 | 2,195,077 | |
| 2024 | 1,474,396 | |
| Thereafter | 2,772,575 | |
| Total | $ | 13,779,023 | |
Total rent expense for the years ended December 31, 2019 and 2018 was $3,381,825 and $2,844,010, respectively.
During the fourth quarter of 2019, the Company entered into various operating leases for its new corporate clinics' space that have not yet commenced. These leases are expected to result in additional ROU asset and liability of approximately $1.3 million. These leases are expected to commence during the first quarter of 2020, with a lease term of five to ten years.
Litigation
In the normal course of business, the Company is party to litigation from time to time. The Company maintains insurance to cover certain actions and believes that resolution of such litigation will not have a material adverse effect on the Company.
Note 13: Segment Reporting
An operating segment is defined as a component of an enterprise for which discrete financial information is available and is reviewed regularly by the Chief Operating Decision Maker (“CODM”) to evaluate performance and make operating decisions. The Company has identified its CODM as the Chief Executive Officer.
The Company has two operating business segments. The Corporate Clinics segment is comprised of the operating activities of the company-owned or managed clinics. As of December 31, 2019, the Company operated or managed 60 clinics under this segment. The Franchise Operations segment is comprised of the operating activities of the franchise business unit. As of December 31, 2019, the franchise system consisted of 453 clinics in operation. Corporate is a non-operating segment that develops and implements strategic initiatives and supports the Company’s two operating business segments by centralizing key administrative functions such as finance and treasury, information technology, insurance and risk management, legal and
human resources. Corporate also provides the necessary administrative functions to support the Company as a publicly-traded company. A portion of the expenses incurred by Corporate are allocated to the operating segments.
The tables below present financial information for the Company’s two operating business segments (in thousands).
| | | | | | | | | | | |
| Year Ended December 31, | | |
| 2019 | | 2018 |
| | | (as adjusted) |
| Revenues: | | | |
| Corporate clinics | $ | 25,808 | | | $ | 19,545 | |
| Franchise operations | 22,643 | | | 17,116 | |
| Total revenues | $ | 48,451 | | | $ | 36,661 | |
| | | |
| Segment operating income: | | | |
| Corporate clinics | $ | 3,365 | | | $ | 1,475 | |
| Franchise operations | 10,975 | | | 8,083 | |
| Total segment operating income | $ | 14,340 | | | $ | 9,558 | |
| | | |
| Depreciation and amortization: | | | |
| Corporate clinics | $ | 1,708 | | | $ | 1,105 | |
| Franchise operations | — | | | — | |
| Corporate administration | 191 | | | 451 | |
| Total depreciation and amortization | $ | 1,899 | | | $ | 1,556 | |
| | | |
| Reconciliation of total segment operating income to consolidated earnings before income taxes: | | | |
| Total segment operating income | $ | 14,340 | | | $ | 9,558 | |
| Unallocated corporate | (10,925) | | | (9,415) | |
| Consolidated income from operations | 3,415 | | | 143 | |
| Bargain purchase gain | 19 | | | 13 | |
| Other (expense), net | (62) | | | (47) | |
| Income before income tax expense | $ | 3,372 | | | $ | 109 | |
| | | | | | | | | | | |
| December 31, 2019 | | December 31, 2018 |
| Segment assets: | | | (as adjusted) |
| Corporate clinics | $ | 25,625 | | | $ | 8,828 | |
| Franchise operations | 5,770 | | | 4,455 | |
| Total segment assets | $ | 31,395 | | | $ | 13,283 | |
| | | |
| Unallocated cash and cash equivalents and restricted cash | $ | 8,642 | | | $ | 8,855 | |
| Unallocated property and equipment | 2,555 | | | 487 | |
| Other unallocated assets | 1,114 | | | 803 | |
| Total assets | $ | 43,706 | | | $ | 23,428 | |
“Unallocated cash and cash equivalents and restricted cash” relates primarily to corporate cash and cash equivalents and restricted cash (see Note 1), “unallocated property and equipment” relates primarily to corporate fixed assets, and “other unallocated assets” relates primarily to deposits, prepaid and other assets.
Note 14: Subsequent Events
On February 28, 2020, the Company entered into a Credit Agreement (the “Credit Agreement”), with JPMorgan Chase Bank, N.A., individually, and as Administrative Agent and Issuing Bank (“JPMorgan Chase” or the “Lender”). The Credit Agreement provides for senior secured credit facilities (the "Credit Facilities") in the amount of $7,500,000, including a $2,000,000 revolver (the "Revolver") and $5,500,000 development line of credit (the "Line of Credit"). The Revolver includes amounts available for letters of credit of up to $1,000,000 and an uncommitted additional amount of $2,500,000 All outstanding principal and interest on the Revolver are due on February 28, 2022. Principal and interest outstanding on the Line of Credit at the end of the first year are converted to a term loan payable in 36 monthly payments with a final maturity date of March 31, 2024. Principal and interest outstanding on the Line of Credit at the end of the second year are converted to a second term loan payable in 36 monthly payments with a final maturity date of March 31, 2025. Borrowings under the Credit Facilities bear interest at a rate equal to an applicable margin, which is a one-, three- or six-month reserve adjusted Eurocurrency rate plus 2.00% or, at the election of the Company, an alternative base rate, plus 1.00%. The alternative base rate is the greatest of the prime rate, the Federal Reserve Bank of New York rate plus 0.50% and the one-month reserve adjusted Eurocurrency plus 1.00%. Unused portions of the Credit Facilities bear interest at a rate equal to 0.25% per annum. If the current Eurocurrency rate is no longer available or representative, the loan agreement provides a mechanism for replacing that benchmark rate. The Credit Facilities are pre-payable at any time without penalty, other than customary breakage fees, and any voluntary repayments made by the Company would reduce the future required repayment amounts.
The Credit Facilities contain customary events of default, including but not limited to nonpayment; material inaccuracy of representations and warranties; violations of covenants; certain bankruptcies and liquidations; cross-default to material indebtedness; certain material judgments; and certain fundamental changes such as a merger or sale of substantially all assets (as further defined in the Credit Facilities). The Credit Facilities require the Company to comply with customary affirmative, negative and financial covenants, including minimum interest coverage and maximum net leverage. A breach of any of these operating or financial covenants would result in a default under the Credit Facilities. If an event of default occurs and is continuing, the lenders could elect to declare all amounts then outstanding, together with accrued interest, to be immediately due and payable. The Credit Facilities are collateralized by substantially all of the Company’s assets, including the assets in the Company’s company-owned or managed clinics. The Company intends to use the Revolver for general working capital needs and the Line of Credit for acquiring and developing new chiropractic clinics.
The Company granted a security interest to the Lender in all assets of the Company, including the assets in the Company’s company-owned or managed clinics, and all proceeds thereof, pursuant to a pledge and security agreement.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
We conducted an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures as of December 31, 2019. Disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act) are designed to provide reasonable assurance that information required to be disclosed in our reports filed under the Exchange Act, such as this Annual Report on Form 10-K, is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures also include, without limitation, controls and procedures that are designed to provide reasonable assurance that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure.
The evaluation of our disclosure controls and procedures included a review of the control objectives and design, our implementation of the controls and the effect of the controls on the information generated for use in this Annual Report on Form 10-K. After conducting this evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures, as defined by Rule 13a-15(e) under the Exchange Act, were not effective as of December 31, 2019 due to a material weakness in internal control over financial reporting, described below.
Management's Report on Internal Control Over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rule 13a-15(f) of the Exchange Act). Internal control over financial reporting is the process designed under the Chief Executive Officer’s and the Chief Financial Officer’s supervision, and effected by our Board of Directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles in the United States.
There are inherent limitations in the effectiveness of internal control over financial reporting, including the possibility that misstatements may not be prevented or detected. Accordingly, an effective control system, no matter how well designed and operated, can provide only reasonable assurance of achieving the designed control objectives, and management is required to apply its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, within the Company have been detected. The design of any system of controls is also based in part upon certain assumptions about the likelihood of future events, and there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions.
Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2019, as required by Exchange Act Rule 13a-15(c). In making this assessment, we used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”) in the 2013 Internal Control - Integrated Framework (2013 Framework). A material weakness is a deficiency, or a combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of our annual or interim financial statements will not be prevented or detected on a timely basis.
We identified a material weakness in internal control related to ineffective information technology general controls (ITGCs) in the areas of user access, information security policies, and program change-management over certain information technology (IT) systems that support the Company’s financial reporting processes. We believe that these control deficiencies were a result of: IT control processes lacking sufficient documentation; and risk-assessment processes inadequate to identify and assess changes in IT environments that could impact internal control over financial reporting. The material weakness did not result in any identified misstatements to the financial statements. Based on this material weakness, the Company’s management concluded that as of December 31, 2019, the Company’s internal control over financial reporting was not effective.
Our independent registered public accounting firm, Plante Moran, PLLC has issued an adverse opinion with respect to the effectiveness of the Company's internal control over financial reporting, which appears in Item 8 of this Form 10-K. Following identification of the material weakness and prior to filing this Form 10-K, we completed substantive procedures for the year ended December 31, 2019. Based on these procedures, management believes that our consolidated financial statements included in this Form 10-K have been prepared in accordance with U.S. GAAP. Our Chief Executive Officer and Chief Financial Officer have certified that, based on their knowledge, the financial statements, and other financial information included in this Form 10-K, fairly present in all material respects the financial condition, results of operations and cash flows of the Company as of, and for, the periods presented in this Form 10-K. Plante Moran, PLLC has issued an unqualified opinion on our financial statements, which is included in Item 8 of this Form 10-K.
Remediation Plan for Material Weakness in Internal Control over Financial Reporting
Management has been implementing and continues to implement measures designed to ensure that control deficiencies contributing to the material weakness are remediated, such that these controls are designed, implemented, and operating effectively. The remediation actions include: (i) updating our IT policies addressing ITGCs; (ii) educating control owners concerning the principles and requirements of each control, with a focus on those related to user access and change-management over IT systems impacting financial reporting; (iii) developing and maintaining documentation underlying ITGCs; (iv) developing enhanced risk assessment procedures and controls related to changes in IT systems; and (v) enhanced quarterly reporting on the remediation measures to the Audit Committee of the Board of Directors. We believe that these actions will remediate the material weakness. The weakness will not be considered remediated, however, until the applicable controls operate for a sufficient period of time and management has concluded, through testing, that these controls are operating effectively. We expect that the remediation of this material weakness will be completed during fiscal 2020 and we plan to monitor these changes throughout the year to ensure that new controls are operating effectively.
Changes in Internal Controls over Financial Reporting
During the first quarter of 2019, we implemented new controls in connection with our adoption of ASC 842. Other than the material weakness in our internal control over financial reporting described above, no other changes in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) occurred during the year ended December 31, 2019 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
ITEM 9B. OTHER INFORMATION
None.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by this item will be included in our Proxy Statement to be filed pursuant to Regulation 14A within 120 days after our year ended December 31, 2019 in connection with our 2020 Annual Meeting of Stockholders, or the 2020 Proxy Statement, and is incorporated herein by reference.
Code of Business Conduct and Ethics
We have adopted a Code of Business Conduct and Ethics that applies to employees, officers and directors, including our executive management team, such as our Chief Executive Officer and Chief Financial Officer. This Code of Business Conduct and Ethics is posted on our website at www.thejoint.com. We intend to satisfy the requirements under Item 5.05 of Form 8-K regarding disclosure of amendments to, or waivers from, provisions of the Code of Business Conduct and Ethics by posting such information on our website.
ITEM 11. EXECUTIVE COMPENSATION
The information required by this item will be included in the 2020 Proxy Statement and is incorporated herein by reference.
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this Item will be included in the 2020 Proxy Statement and is incorporated herein by reference.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this item will be included in the 2020 Proxy Statement and is incorporated herein by reference.
ITEM 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES
The information required by this item will be included in the 2020 Proxy Statement and is incorporated herein by reference.
PART IV
ITEM 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES
(a)Documents filed as part of this report.
(1)Financial Statements. The consolidated financial statements listed on the index to Item 8 of this Annual Report on Form 10-K are filed as a part of this Annual Report.
(2)Financial Statement Schedules. All financial statement schedules have been omitted since the information is either not applicable or required or is included in the financial statements or notes thereof.
(3)Exhibits. Those exhibits marked with a (X) refer to exhibits filed or furnished herewith. The other exhibits are incorporated herein by reference, as indicated in the following list. Those exhibits marked with a (#) refer to management contracts or compensatory plans or arrangements. Portions of the exhibits marked with a (Ω) are the
subject of a Confidential Treatment Request under 17 C.F.R. §§ 200.80(b)(4), 200.83 and 240.24b-2. Omitted material for which confidential treatment has been requested has been filed separately with the SEC.
EXHIBIT INDEX
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | Incorporated by Reference | | | | | | | |
Exhibit
Number | | Description | | Form | | File No. | | Exhibit(s) | | Filing Date | Provided
Herewith |
| 3.1 | | | | | S-1 | | 333-198860 | | 3.2 | | | 9/19/2014 | |
| 3.2 | | | | | 8-K | | 001-36724 | | 3(ii).1 | | 3/7/2016 | |
| 3.3 | | | | | 8-K | | 001-36724 | | 3.(II)1 | | 8/9/2018 | |
| 4.1 | | | | | | | | | | | | X |
| 10.1# | | | | S-1 | | 333-198860 | | 10.1 | | | 9/19/2014 | |
| 10.2# | | | | S-1 | | 333-198860 | | 10.18 | | | 9/19/2014 | |
| 10.3# | | | | S-1 | | 333-198860 | | 10.19 | | | 9/19/2014 | |
| 10.4# | | | | S-1 | | 333-198860 | | 10.2 | | | 9/19/2014 | |
| 10.5# | | | | S-1 | | 333-207632 | | 10.3 | | | 10/27/2015 | |
| 10.6# | | | | | | | | | | | X |
| 10.7# | | | | S-1 | | 333-207632 | | 10.4 | | | 10/27/2015 | |
| 10.8# | | | | 8-K | | 333-207632 | | 10.1 | | | 4/3/2019 | |
| 10.9# | | | | | | | | | | | X |
| 10.10# | | | | S-1 | | 333-207632 | | 10.5 | | | 10/27/2015 | |
| 10.11# | | | | 8-K | | 333-207632 | | 10.2 | | | 4/3/2019 | |
| 10.12# | | | | | | | | | | | X |
| 10.13# | | | | S-1 | | 333-207632 | | 10.6 | | | 10/27/2015 | |
| 10.14# | | | | 10-K | | 001-36724 | | 10.54 | | | 3/9/2018 | |
| 10.15# | | | | 8-K | | 333-207632 | | 10.3 | | | 4/3/2019 | |
| 10.16# | | | | | | | | | | | | | X |
| 10.17# | | | | | 10-K | | 001-36724 | | 10.53 | | | 3/9/2018 | |
| 10.18# | | | | | 10-K | | 001-36724 | | 10.11 | | | 3/11/2019 | |
| 10.19 | | | | | 10-K | | 001-36724 | | 10.12 | | | 3/11/2019 | |
| 10.20 | | | | | | | | | | | | X |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| 10.21 | | | | | S-1 | | 333-198860 | | 10.13 | | | 9/19/2014 | |
| 10.22 | | | | | S-1 | | 333-198860 | | 10.14 | | | 9/19/2014 | |
| 10.23 | | | | | S-1 | | 333-198860 | | 10.15 | | | 9/19/2014 | |
| 10.24 | | Asset Purchase Agreement dated July 17, 2019, by and among The Joint Corp., TJ of Savannah – Twelve Oaks, LLC, a Georgia limited liability company, TJ of Pooler, LLC, a Georgia limited liability company, and TJ of Bluffton, LLC, a Georgia limited liability company , Robyn Meglin and Allen Meglin, as amended | | 8-K | | 001-36724 | | 10.1 | | | 7/23/2019 | |
| 10.25 | | | | 8-K | | 001-36724 | | 10.1 | | | 8/5/2019 | |
| 10.26 | | | | 8-K | | 001-36724 | | 10.1 | | | 8/19/2019 | |
| 10.27 | | | | 8-K | | 001-36724 | | 10.1 | | | 1/9/2017 | |
| 10.28 | | | | 8-K | | 001-36274 | | 10.2 | | | 1/9/2017 | |
| 10.29 | | | | 8-K | | 001-36274 | | 10.2 | | 1/9/2017 | |
| 10.30# | | | | | 8-K | | 001-36724 | | 10.1 | | | 11/8/2018 | |
| 10.31# | | | | | 8-K | | 001-36724 | | 10.2 | | | 11/8/2018 | |
| 10.32# | | | | | | | | | | | | | X |
| 10.33# | | | | | 8-K | | 001-36724 | | 10.1 | | | 5/3/2016 | |
| 10.34# | | | | | 8-K | | 001-36274 | | 10.3 | | | 1/9/2017 | |
| 10.35# | | | | | 8-K | | 001-36724 | | 10.1 | | | 12/6/2018 | |
| 10.36# | | | | | 10-K | | 001-36724 | | 10.4 | | | 3/11/2019 | |
| 16 | | | | | 8-K | | 001-36724 | | 16.1 | | | 10/4/2018 | |
| 21 | | | | | S-1 | | 333-198860 | | 21.1 | | | 9/19/2014 | |
| 23.1 | | | | | | | | | | | | X |
| 31.1 | | | | | | | | | | | | X |
| | | | | | | | |
| 101.INS | XBRL Instance Document | X |
| 101.SCH | XBRL Taxonomy Extension Schema Document | X |
| 101.CAL | XBRL Taxonomy Extension Calculation Linkbase Document | X |
| 101.DEF | XBRL Taxonomy Extension Definition Linkbase Document | X |
| 101.LAB | XBRL Taxonomy Extension Label Linkbase Document | X |
| 101.PRE | XBRL Taxonomy Extension Presentation Linkbase Document | X |
| # Management contract or compensatory plan or arrangement | | |
| ** Furnished, not filed | | |
___________________
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized on March 6, 2020.
| | | | | | | | |
| The Joint Corp. | |
| | |
| By: | /s/ Jake Singleton |
| | Jake Singleton Chief Financial Officer
(Principal Financial Officer) |
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Peter D. Holt and Jake Singleton, jointly and severally, his or her attorneys-in-fact, each with the power of substitution, for him or her in any and all capacities, to sign any amendments to this Report on Form 10-K, and to file the same, with exhibits thereto and other documents in connection therewith with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact, or his or her substitute or substitutes may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons in the capacities and on the dates indicated.
| | | | | | | | | | | | | | |
| Signature | | Title | | Date |
| | | | |
| /s/ Peter D. Holt | | President, Chief Executive Officer and Director | | March 6, 2020 |
| Peter D. Holt | | (Principal Executive Officer) and Director | | |
| | | | |
| /s/ Jake Singleton | | Chief Financial Officer | | March 6, 2020 |
| Jake Singleton | | (Principal Financial Officer) | | |
| | | | |
| /s/ Matthew E. Rubel | | Lead Director | | March 6, 2020 |
| Matthew E. Rubel | | | | |
| | | | |
| /s/ James H. Amos, Jr. | | Director | | March 6, 2020 |
| James H. Amos, Jr. | | | | |
| | | | |
| /s/ Ronald V. DaVella | | Director | | March 6, 2020 |
| Ronald V. DaVella | | | | |
| | | | |
| /s/ Suzanne M. Decker | | Director | | March 6, 2020 |
| Suzanne M. Decker | | | | |
| | | | |
| /s/ Abe Hong | | Director | | March 6, 2020 |
| Abe Hong | | | | |
| | | | |
| /s/ Glenn J. Krevlin | | Director | | March 6, 2020 |
| Glenn J. Krevlin | | | | |